فیبرین غنی از پلاکت تزریقی (i-PRF) به عنوان یک ابزار بیولوژیک و نوین در پزشکی بازساختی، بهویژه در حوزه ارتوپدی، توجه زیادی را به خود جلب کرده است. این ماده یک فرآورده اتولوگ تمرکزیافته پلاکتی است که از طریق یک فرآیند سانتریفیوژ ساده، کوتاه و بدون نیاز به افزودنیهای ضدانعقاد از خون خود بیمار به دست میآید. ساختار بیولوژیکی i-PRF شامل یک ماتریکس مایع غنی از فیبرین، لکوسیتها (گلبولهای سفید) و فاکتورهای رشد متعدد (مانند VEGF، PDGF، TGF-β و FGF) است. این اجزا در کنار هم باعث تحریک تکثیر سلولی، رگزایی (آنژیوژنز) و پاسخهای ضدالتهابی قدرتمند میشوند که آن را برای ترمیم بافتهای استخوانی، غضروفی و همچنین به عنوان سیستمهای هوشمند انتقال دارو ایدهآل میسازد.
مزیت کلیدی i-PRF نسبت به پلاسمای غنی از پلاکت سنتی (PRP)، رهاسازی تدریجی و طولانیمدت فاکتورهای رشد (تا ۱۴ روز) به دلیل ساختار ماتریکس فیبرینی آن است. علاوه بر این، i-PRF دارای خواص ضدباکتریایی مؤثری علیه پاتوژنهای شایع بوده و میتواند قطبش ماکروفاژها را از حالت التهابی (M1) به حالت ترمیمی و ضدالتهابی (M2) تغییر دهد. در درمان آرتروز زانو، این فرآورده با کاهش سیتوکینهای پیشالتهابی، درد بیماران را کاهش داده و عملکرد مفصل را بهبود میبخشد. با وجود پتانسیل بالا، چالشهایی مانند کنترل دقیق نرخ رهاسازی فاکتورها و پایداری دارویی در ماتریکس همچنان نیازمند بررسی بیشتر است. این مقاله به بررسی جامع تاریخچه، مکانیسمهای سلولی، کاربردهای بالینی، مقرونبهصرفه بودن و نسلهای جدید فرآوردههای PRF (مانند A-PRF، T-PRF و C-PRF) میپردازد.
The Role of Injectable Platelet-Rich Fibrin in Orthopedics: Where Do We Stand?
Abstract
Injectable Platelet-Rich Fibrin (i-PRF) has emerged as a highly promising autologous biomaterial in regenerative medicine, particularly within the field of orthopedics. Obtained through a simple, low-speed, and anticoagulant-free centrifugation process, i-PRF yields a liquid matrix enriched with a high concentration of platelets, leukocytes, and essential growth factors. These biological components actively promote tissue regeneration, accelerate angiogenesis, modulate inflammatory responses, and provide notable antimicrobial defenses. This comprehensive review explores the development, biological mechanisms, and orthopedic clinical applications of i-PRF, specifically highlighting its bone and cartilage remodeling capabilities. Furthermore, it contrasts i-PRF with traditional platelet concentrates like Platelet-Rich Plasma (PRP) and Bone Marrow Aspirate Concentrate (BMAC) in terms of efficacy, sustained growth factor delivery, and cost-effectiveness. Finally, current challenges, drug-delivery system integration, and next-generation PRF formulations are discussed to guide future therapeutic optimization.
1. Introduction and Historical Evolution
Platelet concentrates have evolved significantly since their inception. First-generation formulations, predominantly Platelet-Rich Plasma (PRP), required the use of chemical anticoagulants to maintain a liquid state prior to application. However, the incorporation of anticoagulants can hinder the maximization of the natural healing cascade, as coagulation is a fundamental and essential step in tissue repair.
To address these limitations, Platelet-Rich Fibrin (PRF) was introduced as a second-generation platelet concentrate. It was initially conceived and investigated in 2001 by Choukroun and colleagues for oral and maxillofacial surgical procedures due to its absolute simplicity, cost-effectiveness, and ease of handling. Traditional PRF forms a dense, solid fibrin matrix holding leukocytes and healing proteins, acting as an effective alternative to conventional bone grafts.
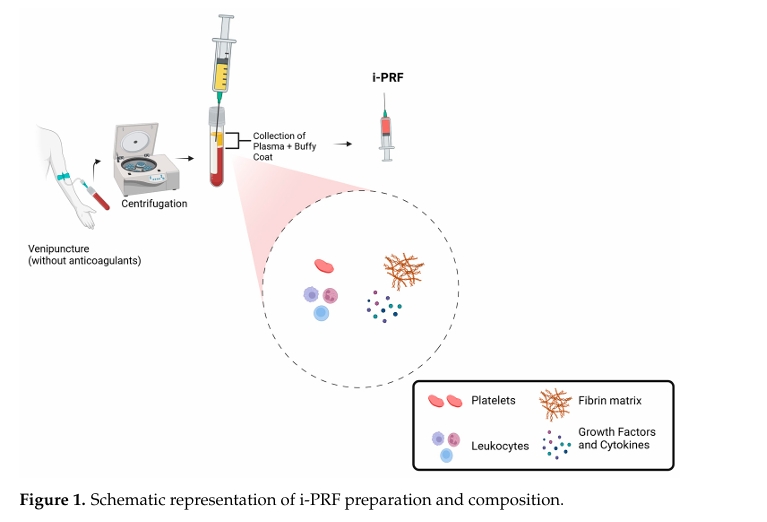
Because standard PRF naturally coagulates rapidly during centrifugation, modifications were necessary to expand its utility to clinical indications requiring an injectable modality. By reducing centrifugation speeds, researchers successfully produced a liquid, non-coagulated version of PRF, termed Injectable PRF (i-PRF). Developed and systematically investigated in 2015, the original protocol utilized a very short, slow centrifugation concept at 700 rpm ($60\text{ G}$) for 3 to 4 minutes within plastic tubes. This liquid form preserves temporary liquid fibrinogen and thrombin that have not yet converted into a cross-linked fibrin clot, granting it superior wound-healing and clotting abilities upon tissue infiltration.
Modern horizontal centrifugation techniques have further optimized cell collection. While fixed-angle devices restrict optimal separation, horizontal centrifugation has demonstrated up to a fourfold increase in cell concentrations. Today, a widely accepted protocol involves collecting 10 mL of venous blood in a dry glass or plastic tube without anticoagulants, followed by centrifugation for 5 to 8 minutes at $60\text{ G}$. This isolates an upper liquid layer that concentrates 2 to 3 times more platelets and a 23% increase in leukocytes compared to whole blood.
2. Biological Properties and Mechanisms of Action
[Venipuncture (No Anticoagulants)]
│
▼
[Low-Speed Centrifugation (5-8 min @ 60 G)]
│
▼
[Collection of Plasma + Buffy Coat Layer] ──► [Injectable i-PRF Liquid]
│
┌────────────────────┴────────────────────┐
▼ ▼
[Bioactive Components] [Sustained Matrix]
• Platelets & Leukocytes • Fibrin Scaffold
• Growth Factors (VEGF, PDGF, TGF-β, FGF) • Gradual 14-day Release
2.1. Growth Factors and Tissue Regeneration
The therapeutic potency of i-PRF lies in its rich composition of bioactive factors embedded within a dynamic matrix. The primary growth factors clustered in i-PRF include:
-
Platelet-Derived Growth Factor (PDGF): Drives cell proliferation and migration.
-
Transforming Growth Factor Beta (TGF-β): Directs cellular differentiation and matrix synthesis.
-
Fibroblast Growth Factor (FGF): Supports tissue remodeling and cellular activity.
-
Vascular Endothelial Growth Factor (VEGF): Acts as a primary mediator of neovascularization.
The raw fibrin matrix mimics the natural extracellular matrix, functioning as a bioactive scaffold that actively guides cell proliferation, migration, and differentiation to the injury site.
2.2. Angiogenesis and Neovascularization
Adequate blood supply is vital to supply the metabolic requirements, oxygen, and nutrients needed for tissue repair. The fibrin architecture of i-PRF stimulates profound angiogenesis by continuously releasing angiogenic growth factors, primarily VEGF. This process of neovascularization ensures a healthy exchange of metabolites and gases, allowing the orderly progression of the healing cascade.
2.3. Anti-Inflammatory Properties and Macrophage Polarization
Chronic or excessive inflammation can cause extensive tissue damage and delay repair . i-PRF directly modulates inflammatory pathways by downregulating pro-inflammatory cytokines, such as Interleukin-1 beta ($\text{IL-1}\beta$) and Tumor Necrosis Factor-alpha ($\text{TNF}-\alpha$). Concurrently, it upregulates anti-inflammatory cytokines like Interleukin-10 ($\text{IL-10}$).
A pivotal property of i-PRF is its ability to promote macrophage polarization, shifting macrophages from the pro-inflammatory M1 phenotype to the anti-inflammatory, regenerative M2 phenotype. In vitro studies (e.g., Nasirzade et al.) established that exposing primary murine and human macrophage cell lines to inflammatory stimuli alongside PRF lysates substantially lowered the expression of pro-inflammatory M1 markers ($\text{IL-1}\beta$ and $\text{IL-6}$), while significantly increasing tissue resolution markers.
2.4. Antibacterial Defenses
Infections present severe complications in orthopedic procedures . i-PRF exhibits inherent antibacterial properties, effectively inhibiting pathogens commonly associated with surgical site infections, including Escherichia coli, Staphylococcus aureus, and Pseudomonas aeruginosa. This antimicrobial action is driven by:
-
The presence of natural antibacterial factors, such as lysozyme.
-
Active immune sentinels within the matrix, specifically leukocytes (neutrophils and lymphocytes) that eliminate invading pathogens.
-
The structural formation of a localized physical barrier that prevents bacterial proliferation.
3. i-PRF as a Pharmacological Carrier (Drug Delivery System)
Beyond its standalone biological benefits, i-PRF’s unique fibrin matrix serves as an excellent drug delivery platform for localized and sustained delivery of antibiotics, anti-inflammatory agents, and additional growth factors. This targeted delivery optimizes therapeutic efficacy directly at the lesion site while minimizing systemic adverse side effects.
| Parameter | Platelet-Rich Plasma (PRP) | Injectable Platelet-Rich Fibrin (i-PRF) |
| Fibrin Matrix Scaffold |
Absent |
Flexible, rich, and highly structured |
| Release Kinetics |
Rapid burst release (minutes to hours) |
Gradual, prolonged release (up to 14 days) |
| Mechanism | Rapid flow of elements due to lack of physical retention |
Scaffold acting like architectural reinforcement bars, restricting free molecular movement to guarantee steady release |
Despite these benefits, several clinical integration challenges remain:
-
Drug Stability: The biochemical properties of the changing fibrin matrix can alter the structural stability of the embedded drug.
-
Release Control Rate: Managing a precise release rate amid a complex, changing biological microenvironment proves difficult.
-
Bioactive Interactions: Potential cross-interference between incorporated pharmacological agents and endogenous cytokines, growth factors, or cells may alter both drug performance and i-PRF matrix behavior.
4. Orthopedic Applications
4.1. Bone Regeneration and Graft Enhancement
Bone regeneration requires a highly coordinated sequence of osteogenic differentiation, angiogenesis, and extracellular matrix remodeling . i-PRF acts as a potent biologically active scaffold that enhances bone healing by extending the bioavailability of key osteoinductive molecules like PDGF, VEGF, TGF-β, and bone morphogenetic proteins (BMPs).
At the molecular level, i-PRF drives bone matrix mineralization and osteoblast activity through specific signaling pathways:
-
Transcription Upregulation: Significantly upregulates $\text{RUNX2}$ and $\text{Osterix}$, which are essential transcription factors for osteoblast differentiation.
-
Pathway Activation: Enhances the canonical $\text{Wnt}/\beta\text{-catenin}$ signaling pathway, a crucial regulator of skeletal development and bone formation.
-
Angiogenic Pathway Integration: Activates the hypoxia-inducible factor-1 alpha ($\text{HIF-1}\alpha$) pathway, which accelerates angiogenesis within the bone microenvironment to deliver necessary nutrients to regenerating tissue.
When combined with bone grafts, i-PRF acts as a clinical potentiator, accelerating bone formation, increasing newly formed bone density, and improving overall graft consolidation and integration. Clinical applications include maxillary sinus augmentations, repair of post-extraction bone defects, and complex fracture repairs.
4.2. Cartilage Repair and Osteoarthritis Management
Articular cartilage possesses a limited intrinsic self-repair capacity. In experimental models of osteoarthritis, i-PRF has shown superior regenerative properties over PRP by significantly promoting chondrocyte proliferation and upregulating key chondrogenic marker mRNA levels, including $\text{Sox9}$, type II collagen, and aggrecan.
i-PRF serves as an active microenvironment that recruits and retains mesenchymal stem cells (MSCs) at cartilage injury sites, driving chondrogenesis via the activation of $\text{TGF}-\beta$ and $\text{Wnt}/\beta\text{-catenin}$ pathways. It also upregulates Insulin-like Growth Factor-1 ($\text{IGF-1}$) and Bone Morphogenetic Protein 2 ($\text{BMP2}$), which stimulate proteoglycan synthesis while suppressing the catabolic enzymes responsible for cartilage degradation.
Clinical data regarding knee osteoarthritis show substantial reductions in pain and clear improvements in joint functionality. Compared to hyaluronic acid—which primarily provides mechanical joint lubrication—i-PRF delivers combined anti-inflammatory and regenerative advantages. Furthermore, preclinical knee models utilizing critical-sized osteochondral defects confirmed that i-PRF outperforms PRP in overall osteochondral tissue regeneration. Emerging therapies also look to combine i-PRF with hyaluronic acid or stem cells to generate synergistic benefits for joint lubrication and cartilage repair.
5. Comparative Overview of Biologics (i-PRF vs. PRP vs. BMAC)
To properly position i-PRF within orthobiologics, it must be compared against established treatments like PRP and Bone Marrow Aspirate Concentrate (BMAC).
| Feature | Injectable Platelet-Rich Fibrin (i-PRF) | Platelet-Rich Plasma (PRP) | Bone Marrow Aspirate Concentrate (BMAC) |
| Preparation Method |
Venipuncture and single low-speed centrifugation |
Venipuncture and standard two-step centrifugation |
Bone marrow aspiration (requires Jamshidi needle) and centrifugation |
| Anticoagulant Use |
No |
Yes |
Yes |
| Fibrin Matrix |
Flexible and rich injectable fibrin matrix |
None |
None |
| Cellular Content |
Platelets, leukocytes, cytokines, growth factors |
Platelets, leukocytes, cytokines, growth factors |
Mesenchymal stem cells (MSCs), platelets, growth factors, cytokines |
| Growth Factor Release |
Sustained (up to 14 days) |
Rapid burst (minutes to several hours) |
Varies (highly dependent on donor MSC activity) |
| Inflammatory Modulation |
Strong anti-inflammatory effect |
Moderate anti-inflammatory effect |
Anti-inflammatory and regenerative effects |
| Clinical Applications |
Osteoarthritis, cartilage repair, soft tissue healing |
Osteoarthritis, tendon injuries, sports medicine |
Non-union fractures, bone regeneration, cartilage defects |
| Cost & Invasiveness |
Low cost, minimally invasive blood draw |
Moderate cost, minimally invasive blood draw |
High cost, highly invasive bone extraction |
Note on BMAC Limitations: While BMAC supplies direct mesenchymal stem cells, its regenerative capacity relies heavily on donor cell viability and proliferation capacity, both of which decline significantly with patient age and health status. Conversely, i-PRF functions as an independent bioactive matrix, providing a predictable, continuous release of growth factors regardless of donor cell age limits.
6. Cost-Effectiveness and Clinical Viability
From an economic standpoint, i-PRF offers clear advantages. Its single-centrifugation protocol, short preparation times, reduced material requirements, and reliance on small autologous blood samples drastically lower processing costs compared to complex biological therapies. While centrifuge machinery requires an upfront investment, its mid-term clinical use is highly advantageous. These logistical benefits make i-PRF exceptionally viable for public healthcare settings and resource-limited systems, facilitating widespread adoption for patients suffering from degenerative musculoskeletal disorders.
7. Future Directions: Next-Generation Solid PRF Formulations
To fulfill specific structural or extended-release clinical criteria, modifications to classic protocols have generated solid next-generation PRF formulations:
-
Advanced PRF (A-PRF): Formed via lower centrifugation forces and extended times, this variant yields a porous, flexible fibrin network that traps high concentrations of leukocytes and platelets. This profile maximizes extended growth factor release, making it ideal for bone grafting, non-union fractures, and complex soft tissue healing.
-
Titanium PRF (T-PRF): Prepared in specialized titanium-coated tubes, titanium acts as a potent activator that enhances fibrin polymerization. This creates a dense, highly structured matrix that optimizes cell adhesion and retention during guided tissue regeneration and bone defect repair.
-
Concentrated PRF (C-PRF): Generated by precisely removing excess plasma from the standard PRF clot, C-PRF results in a highly concentrated matrix that delivers a tenfold increase in platelet and leukocyte yields. Its prolonged bioactivity is tailored for chronic wound care and long-term cartilage engineering.
While i-PRF remains uniquely advantageous as the only fully injectable fluid formulation, these solid variations offer useful, three-dimensional therapeutic scaffolds that can complement injectable treatments in complex orthopedic cases.
8. Conclusions
Injectable Platelet-Rich Fibrin (i-PRF) represents a significant advancement in autologous orthobiologics. By eliminating anticoagulants and utilizing slow horizontal centrifugation, it preserves a fluid matrix capable of delivering prolonged, 14-day bioactive stimulation directly to damaged bone and joint tissues. Its validated anti-inflammatory properties, capacity to polarize macrophages toward a regenerative M2 phenotype, inherent antibacterial activity, and high cost-effectiveness highlight its clinical potential. While ongoing research continues to refine standardized centrifugation parameters and explore combination delivery therapies, i-PRF stands as a safe, accessible, and powerful tool destined to expand the reach of regenerative medicine in modern orthopedics.
References
-
Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Dohan, D.M. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part IV: Clinical Effects on Tissue Healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e56-e60. https://doi.org/10.1016/j.tripleo.2005.07.011
-
Toffler, M.; Toscano, N.; Holtzclaw, D.; Corso, M.; Ehrenfest, D.M. Introducing Choukroun’s Platelet Rich Fibrin (PRF) to the Reconstructive Surgery Milieu. J. Implant Adv. Clin. Dent. 2009, 1, 21-32.
-
Diab, N.A.F.; Ibrahim, A.-S.M.; Abdallah, A.M. Fluid Platelet-Rich Fibrin (PRF) Versus Platelet-Rich Plasma (PRP) in the Treatment of Atrophic Acne Scars: A Comparative Study. Arch. Dermatol. Res. 2023, 315, 1249-1255. https://doi.org/10.1007/s00403-022-02498-y
-
Lana, J.F.; Purita, J.; Everts, P.A.; De Mendonça Neto, P.A.T.; de Moraes Ferreira Jorge, D.; Mosaner, T.; Huber, S.C.; Azzini, G.O.M.; da Fonseca, L.F.; Jeyaraman, M.; et al. Platelet-Rich Plasma Power-Mix Gel (Ppm)-An Orthobiologic Optimization Protocol Rich in Growth Factors and Fibrin. Gels 2023, 9, 553. https://doi.org/10.3390/gels9070553
-
Mourão, C.F.D.A.B.; Valiense, H.; Melo, E.R.; Mourão, N.B.M.F.; Maia, M.D.-C. Obtention of Injectable Platelets Rich-Fibrin (i-PRF) and Its Polymerization with Bone Graft: Technical Note. Rev. Col. Brasileiro Cir. 2015, 42, 421-423. https://doi.org/10.1590/0100-69912015006013
-
Miron, R.J.; Fujioka-Kobayashi, M.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Ghanaati, S.; Choukroun, J. Injectable Platelet Rich Fibrin (i-PRF): Opportunities in Regenerative Dentistry? Clin. Oral Investig. 2017, 21, 2619-2627. https://doi.org/10.1007/s00784-017-2063-9
-
Miron, R.J.; Chai, J.; Zheng, S.; Feng, M.; Sculean, A.; Zhang, Y. A Novel Method for Evaluating and Quantifying Cell Types in Platelet Rich Fibrin and an Introduction to Horizontal Centrifugation. J. Biomed. Mater. Res. A 2019, 107, 2257-2271. https://doi.org/10.1002/jbm.a.36735
-
Dashore, S.; Chouhan, K.; Nanda, S.; Sharma, A. Platelet-Rich Fibrin, Preparation and Use in Dermatology. Indian Dermatol. Online J. 2021, 12, S55-S65. https://doi.org/10.4103/idoj.idoj_267_21
-
Miron, R.J.; Chai, J.; Fujioka-Kobayashi, M.; Sculean, A.; Zhang, Y. Evaluation of 24 Protocols for the Production of Platelet-Rich Fibrin. BMC Oral Health 2020, 20, 310. https://doi.org/10.11607/jomi.8443
-
dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The Regenerative Mechanisms of Platelet-Rich Plasma: A Review. Cytokine 2021, 144, 155560. https://doi.org/10.1016/j.cyto.2021.155560
-
Pan, J.; Luo, L.; Jiang, Z.; Huang, H.; Jiang, B. The Effect of Injectable Platelet-Rich Fibrin and Platelet-Rich Fibrin in Regenerative Endodontics: A Comparative in Vitro Study. J. Appl. Oral Sci. 2024, 32, e20230449. https://doi.org/10.1590/1678-7757-2023-0449
-
Johnson, K.E.; Wilgus, T.A. Vascular Endothelial Growth Factor and Angiogenesis in the Regulation of Cutaneous Wound Repair. Adv. Wound Care 2014, 3, 647-661. https://doi.org/10.1089/wound.2013.0517
-
Balbino, C.A.; Pereira, L.M.; Curi, R. Mecanismos envolvidos na cicatrização: Uma revisão. Rev. Bras. Cienc. Farm. 2005, 41, 27-51. https://doi.org/10.1590/S1516-93322005000100004
-
Nasirzade, J.; Kargarpour, Z.; Hasannia, S.; Strauss, F.J.; Gruber, R. Platelet-rich Fibrin Elicits an Anti-inflammatory Response in Macrophages in Vitro. J. Periodontol. 2020, 91, 244-252. https://doi.org/10.1002/JPER.19-0216
-
Kargarpour, Z.; Nasirzade, J.; Panahipour, L.; Miron, R.J.; Gruber, R. Liquid PRF Reduces the Inflammatory Response and Osteoclastogenesis in Murine Macrophages. Front. Immunol. 2021, 12, 636427. https://doi.org/10.3389/fimmu.2021.636427
-
Kargarpour, Z.; Nasirzade, J.; Panahipour, L.; Miron, R.J.; Gruber, R. Platelet-Rich Fibrin Decreases the Inflammatory Response of Mesenchymal Cells. Int. J. Mol. Sci. 2021, 22, 11333. https://doi.org/10.3390/ijms222111333
-
Martins, R.A.; Costa, F.R.; Pires, L.; Santos, M.; Santos, G.S.; Lana, J.V.; Costa, B.R.; Santos, N.; de Macedo, A.P.; Kruel, A.; et al. Regenerative Inflammation: The Mechanism Explained from the Perspective of Buffy-Coat Protagonism and Macrophage Polarization. Int. J. Mol. Sci. 2024, 25, 11329. https://doi.org/10.3390/ijms252111329
-
Moraschini, V.; Miron, R.J.; Mourão, C.F.D.A.B.; Louro, R.S.; Sculean, A.; da Fonseca, L.A.M.; Calasans Maia, M.D.; Shibli, J.A. Antimicrobial Effect of Platelet-Rich Fibrin: A Systematic Review of in Vitro Evidence-Based Studies. Periodontology 2000 2024, 94, 131-142. https://doi.org/10.1111/prd.12543
-
Balaji, V.R.; Thiagarajan, R.K.; Niazi, T.M.; Ulaganathan, G.; Manikandan, D. Antimicrobial Effects of Platelet Rich Fibrin: A Systematic Review on Current Evidence of Research. J. Interdiscip. Dent. 2021, 11, 2. https://doi.org/10.4103/jid.jid_31_20
-
Jasmine, S.; Thangavelu, A.; Janarthanan, K.; Krishnamoorthy, R.; Alshatwi, A.A. Antimicrobial and Antibiofilm Potential of Injectable Platelet Rich Fibrin-A Second-Generation Platelet Concentrate Against Biofilm Producing Oral Staphylococcus Isolates. Saudi J. Biol. Sci. 2020, 27, 41-46. https://doi.org/10.1016/j.sjbs.2019.04.014
-
Miron, R.J.; Zhang, Y. Autologous Liquid Platelet Rich Fibrin: A Novel Drug Delivery System. Acta Biomater. 2018, 75, 35-51. https://doi.org/10.1016/j.actbio.2018.05.021
-
Murugan, T.; Nd, J. Injectable Platelet Rich Fibrin (I-PRF) As Novel Vehicle for Local Drug Delivery (LDD) In Periodontal Therapy-In-Vitro Pharmacokinetic Study Pilot Study. J. Surv. Fish. Sci. 2023, 10, 232-242.
-
Mourão, C.F.; Lowenstein, A. The Use of Alb-PRF as a Drug Delivery System for Malignant Lesion Treatment. Rev. Bras. Cancerol. 2023, 69, e-013762. https://doi.org/10.32635/2176-9745.RBC.2023v69n2.3762
-
Narayanaswamy, R.; Patro, B.P.; Jeyaraman, N.; Gangadaran, P.; Rajendran, R.L.; Nallakumarasamy, A.; Jeyaraman, M.; Ramani, P.; Ahn, B.-C. Evolution and Clinical Advances of Platelet-Rich Fibrin in Musculoskeletal Regeneration. Bioengineering 2023, 10, 58. https://doi.org/10.3390/bioengineering10010058
-
Barbon, S.; Stocco, E.; Macchi, V.; Contran, M.; Grandi, F.; Borean, A.; Parnigotto, P.P.; Porzionato, A.; De Caro, R. Platelet-Rich Fibrin Scaffolds for Cartilage and Tendon Regenerative Medicine: From Bench to Bedside. Int. J. Mol. Sci. 2019, 20, 1701. https://doi.org/10.3390/ijms20071701
-
Egle, K.; Skadins, I.; Grava, A.; Micko, L.; Dubniks, V.; Salma, I.; Dubnika, A. Injectable Platelet-Rich Fibrin as a Drug Carrier Increases the Antibacterial Susceptibility of Antibiotic-Clindamycin Phosphate. Int. J. Mol. Sci. 2022, 23, 7407. https://doi.org/10.3390/ijms23137407
-
Murdiastuti, K.; Olivia, N.; Kusumadewi, W.; Sumito, N. In Vitro Osteogenic Potential of Freeze-Dried Homologous Platelet-Rich Plasma. Dent. Hypotheses 2021, 12, 91. https://doi.org/10.4103/denthyp.denthyp_23_21
-
Jang, H.-J.; Yoon, J.-K. The Role of Vasculature and Angiogenic Strategies in Bone Regeneration. Biomimetics 2024, 9, 75. https://doi.org/10.3390/biomimetics9020075
-
de Lima Barbosa, R.; Stellet Lourenço, E.; de Azevedo dos Santos, J.V.; Rodrigues Santiago Rocha, N.; Mourão, C.F.; Alves, G.G. The Effects of Platelet-Rich Fibrin in the Behavior of Mineralizing Cells Related to Bone Tissue Regeneration-A Scoping Review of In Vitro Evidence. J. Funct. Biomater. 2023, 14, 503. https://doi.org/10.3390/jfb14100503
-
Yang, S.; En, L.; Yanwei, G.; Mingguo, W. Platelet-Rich Fibrin Promotes Osteogenic Differentiation of Bone Marrow Mesenchymal Stem Cells through Canonical Wnt/β-Catenin Signaling Pathway. Int. J. Oral Maxillofac. Surg. 2015, 44, e310. https://doi.org/10.1016/j.ijom.2015.08.356
-
Zhang, J.; Gao, P.; Chang, W.-R.; Song, J.-Y.; An, F.-Y.; Wang, Y.-J.; Xiao, Z.-P.; Jin, H.; Zhang, X.-H.; Yan, C.-L. The Role of HIF-1α in Hypoxic Metabolic Reprogramming in Osteoarthritis. Pharmacol. Res. 2025, 213, 107649. https://doi.org/10.1016/j.phrs.2025.107649
-
Lana, J.F.S.D.; da Fonseca, L.F.; Macedo, R.D.R.; Mosaner, T.; Murrell, W.; Kumar, A.; Purita, J.; de Andrade, M.A.P. Platelet-Rich Plasma vs Bone Marrow Aspirate Concentrate: An Overview of Mechanisms of Action and Orthobiologic Synergistic Effects. World J. Stem Cells 2021, 13, 155. https://doi.org/10.4252/wjsc.v13.i2.155
-
Liu, H.; Xia, X.; Li, B. Mesenchymal Stem Cell Aging: Mechanisms and Influences on Skeletal and Non-Skeletal Tissues. Exp. Biol. Med. 2015, 240, 1099-1106. https://doi.org/10.1177/1535370215579384
-
Thamaraiselvan, M.; Jayakumar, N.D. Efficacy of Injectable Platelet-Rich Fibrin (i-PRF) as a Novel Vehicle for Local Drug Delivery in Non-Surgical Periodontal Pocket Therapy: A Randomized Controlled Clinical Trial. J. Adv. Periodontol. Implant Dent. 2024, 16, 94-102. https://doi.org/10.34172/japid.2024.011
-
Fernández-Medina, T.; Vaquette, C.; Ivanovski, S. Systematic Comparison of the Effect of Four Clinical-Grade Platelet Rich Hemoderivatives on Osteoblast Behaviour. Int. J. Mol. Sci. 2019, 20, 6243. https://doi.org/10.3390/ijms20246243
-
Rodríguez Flores, J.; Palomar Gallego, M.A.; Torres García-Denche, J. Plasma Rico En Plaquetas: Fundamentos Biológicos y Aplicaciones En Cirugía Maxilofacial y Estética Facial. Rev. Esp. Cir. Oral Maxilofac. 2012, 34, 8-17. https://doi.org/10.1016/j.maxilo.2011.10.007
-
Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-Rich Plasma: A Milieu of Bioactive Factors. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 429-439. https://doi.org/10.1016/j.arthro.2011.10.018
-
Grecu, A.F.; Reclaru, L.; Ardelean, L.C.; Nica, O.; Ciucă, E.M.; Ciurea, M.E. Platelet-Rich Fibrin and Its Emerging Therapeutic Benefits for Musculoskeletal Injury Treatment. Medicina 2019, 55, 141. https://doi.org/10.3390/medicina55050141
-
Cheeva-akrapan, V.; Turajane, T. The 36-Month Survival Analysis of Conservative Treatment Using Platelet-Rich Plasma Enhanced With Injectable Platelet-Rich Fibrin in Patients With Knee Osteoarthritis. Cureus 2023, 15, e35632. https://doi.org/10.7759/cureus.35632
-
Bai, M.-Y.; Vy, V.P.T.; Tang, S.-L.; Hung, T.N.K.; Wang, C.-W.; Liang, J.-Y.; Wong, C.-C.; Chan, W.P. Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs. Int. J. Mol. Sci. 2023, 24, 12608. https://doi.org/10.3390/ijms241612608
-
Wang, J.; Sun, Y.; Liu, Y.; Yu, J.; Sun, X.; Wang, L.; Zhou, Y. Effects of Platelet-Rich Fibrin on Osteogenic Differentiation of Schneiderian Membrane Derived Mesenchymal Stem Cells and Bone Formation in Maxillary Sinus. Cell Commun. Signal. 2022, 20, 88. https://doi.org/10.1186/s12964-022-00902-1
-
Cheng, B.; Feng, F.; Shi, F.; Huang, J.; Zhang, S.; Quan, Y.; Tu, T.; Liu, Y.; Wang, J.; Zhao, Y.; et al. Distinctive Roles of Wnt Signaling in Chondrogenic Differentiation of BMSCs under Coupling of Pressure and Platelet-Rich Fibrin. Tissue Eng. Regen. Med. 2022, 19, 823-837. https://doi.org/10.1007/s13770-022-00466-4
-
Ashour, S.H.; Mudalal, M.; Al-Aroomi, O.A.; Al-Attab, R.; Li, W.; Yin, L. The Effects of Injectable Platelet-Rich Fibrin and Advanced-Platelet Rich Fibrin on Gingival Fibroblast Cell Vitality, Proliferation, Differentiation. Tissue Eng. Regen. Med. 2023, 20, 1161-1172. https://doi.org/10.1007/s13770-023-00593-y
-
Kargarpour, Z.; Nasirzade, J.; Panahipour, L.; Mitulović, G.; Miron, R.J.; Gruber, R. Platelet-Rich Fibrin Increases BMP2 Expression in Oral Fibroblasts via Activation of TGF-β Signaling. Int. J. Mol. Sci. 2021, 22, 7935. https://doi.org/10.3390/ijms22157935
-
Kwon, H.; Paschos, N.K.; Hu, J.C.; Athanasiou, K. Articular Cartilage Tissue Engineering: The Role of Signaling Molecules. Cell. Mol. Life Sci. 2016, 73, 1173-1194. https://doi.org/10.1007/s00018-015-2115-0
-
Wen, C.; Xu, L.; Xu, X.; Wang, D.; Liang, Y.; Duan, L. Insulin-like Growth Factor-1 in Articular Cartilage Repair for Osteoarthritis Treatment. Arthritis Res. Ther. 2021, 23, 277. https://doi.org/10.1186/s13075-021-02662-0
-
Shiga, Y.; Orita, S.; Kubota, G.; Kamoda, H.; Yamashita, M.; Matsuura, Y.; Yamauchi, K.; Eguchi, Y.; Suzuki, M.; Inage, K.; et al. Freeze-Dried Platelet-Rich Plasma Accelerates Bone Union with Adequate Rigidity in Posterolateral Lumbar Fusion Surgery Model in Rats. Sci. Rep. 2016, 6, 36715. https://doi.org/10.1038/srep36715
-
Jia, K.; You, J.; Zhu, Y.; Li, M.; Chen, S.; Ren, S.; Chen, S.; Zhang, J.; Wang, H.; Zhou, Y. Platelet-Rich Fibrin as an Autologous Biomaterial for Bone Regeneration: Mechanisms, Applications, Optimization. Front. Bioeng. Biotechnol. 2024, 12, 1286035. https://doi.org/10.3389/fbioe.2024.1286035
-
Ryu, D.J.; Jeon, Y.S.; Park, J.S.; Bae, G.C.; Kim, J.; Kim, M.K. Comparison of Bone Marrow Aspirate Concentrate and Allogenic Human Umbilical Cord Blood Derived Mesenchymal Stem Cell Implantation on Chondral Defect of Knee: Assessment of Clinical and Magnetic Resonance Imaging Outcomes at 2-Year Follow-Up. Cell Transplant. 2020, 29, 0963689720943581. https://doi.org/10.1177/0963689720943581
-
Knop, E.; Paula, L.E.D.; Fuller, R. Plasma rico em plaquetas no tratamento da osteoartrite. Rev. Bras. Reumatol. 2016, 56, 152–164. https://doi.org/10.1016/j.rbr.2015.04.002
-
Abd El Raouf, M.; Wang, X.; Miusi, S.; Chai, J.; Mohamed AbdEl-Aal, A.B.; Nefissa Helmy, M.M.; Ghanaati, S.; Choukroun, J.; Choukroun, E.; Zhang, Y.; et al. Injectable-Platelet Rich Fibrin Using the Low Speed Centrifugation Concept Improves Cartilage Regeneration When Compared to Platelet-Rich Plasma. Platelets 2019, 30, 213–221. https://doi.org/10.1080/09537104.2017.1401115
-
Miron, R.J.; Gruber, R.; Farshidfar, N.; Sculean, A.; Zhang, Y. Ten Years of Injectable Platelet-Rich Fibrin. Periodontology 2000 2024, 94, 92–113. https://doi.org/10.1111/prd.12541
-
Kemmochi, M.; Sasaki, S.; Takahashi, M.; Nishimura, T.; Aizawa, C.; Kikuchi, J. The Use of Platelet-Rich Fibrin with Platelet-Rich Plasma Support Meniscal Repair Surgery. J. Orthop. 2018, 15, 711–720. https://doi.org/10.1016/j.jor.2018.05.044
-
Torbjörn Ogéus DC, P. Platelet Rich Fibrin Combined with Hyaluronic Acid in the Treatment of Meniscal Injuries: A Retrospective 1-Year Follow-Up Study. J. Orthop. Sports Med. 2025, 7, 88–95.
-
Egle, K.; Dohle, E.; Hoffmann, V.; Salma, I.; Al-Maawi, S.; Ghanaati, S.; Dubnika, A. Fucoidan/Chitosan Hydrogels as Carrier for Sustained Delivery of Platelet-Rich Fibrin Containing Bioactive Molecules. Int. J. Biol. Macromol. 2024, 262, 129651. https://doi.org/10.1016/j.ijbiomac.2024.129651
-
Saluja, H.; Dehane, V.; Mahindra, U. Platelet-Rich Fibrin: A Second Generation Platelet Concentrate and a New Friend of Oral and Maxillofacial Surgeons. Ann. Maxillofac. Surg. 2011, 1, 53–57. https://doi.org/10.4103/2231-0746.83158
-
Dorjay, K.; Sinha, S. Platelet-Rich Fibrin in Nonhealing Leg Ulcers: A Simple and Effective Therapeutic Option. J. Cutan. Aesthetic Surg. 2021, 14, 160–165. https://doi.org/10.4103/JCAS.JCAS_165_20
-
Elver, A.; Caymaz, M.G. Novel Approaches to the Use of Platelet-Rich Fibrin: A Literature Review. Saudi Dent. J. 2023, 35, 797–802. https://doi.org/10.1016/j.sdentj.2023.07.009
-
Chmielewski, M.; Pilloni, A.; Adamska, P. Application of Advanced Platelet-Rich Fibrin in Oral and Maxillo-Facial Surgery: A Systematic Review. J. Funct. Biomater. 2024, 15, 377. https://doi.org/10.3390/jfb15120377
-
Makki, A.Z.; Alsulami, A.M.; Almatrafi, A.S.; Sindi, M.Z.; Sembawa, S.N. The Effectiveness of Advanced Platelet-Rich Fibrin in Comparison with Leukocyte-Platelet-Rich Fibrin on Outcome after Dentoalveolar Surgery. Int. J. Dent. 2021, 2021, 6686857. https://doi.org/10.1155/2021/6686857
-
Yaşar, N.Ç.; Ünsal, G.; Kocaelli, H.A.; Orhan, K.; Sağ, F.B. Comparative Analysis of Local Application of Titanium-Platelet Rich Fibrin (T-PRF) and Leukocyte-Platelet Rich Fibrin (L-PRF) in Bone Defect Healing: A Micro-CT and Histopathological Study in Rabbit Models. Microsc. Res. Tech. 2025, 88, 1–12. https://doi.org/10.1002/jemt.24715
-
Miron, R.J.; Chai, J.; Zhang, P.; Li, Y.; Wang, Y.; de Almeida Barros Mourão, C.F.; Sculean, A.; Fujioka Kobayashi, M.; Zhang, Y. A Novel Method for Harvesting Concentrated Platelet-Rich Fibrin (C-PRF) with a 10-Fold Increase in Platelet and Leukocyte Yields. Clin. Oral Investig. 2020, 24, 2819–2828. https://doi.org/10.1007/s00784-019-03147-w