آرتروز زانو (OA) یک بیماری تخریبپذیر مزمن است که با درد، کاهش تحرک و کاهش کیفیت زندگی همراه است. درمانهای مرسوم اغلب با هدف تسکین موقت یا تعویض مفصل انجام میشوند. هدف این مطالعه ارزیابی اثربخشی بالینی تزریق درونمفصلی «استرومای غنی از پلاکت» (PRS) — ترکیبی از پلاسمای غنی از پلاکت (PRP) و فرکشن واسکولار استرومال بافتی (tSVF) به صورت مکانیکی — در درمان بیماران مبتلا به آرتروز زانو (گرید ۲ و ۳ کیلگرن-لاورنس) است. در یک مطالعه مجموعه موارد متوالی (Case Series)، ۱۵ بیمار (بین ۴۳ تا ۷۵ سال) با یکبار تزریق اتولوگ PRS درمان شدند. ارزیابیهای بالینی با استفاده از معیارهای تفکیک بالینی VAS (درد)، WOMAC (درد، سفتی و عملکرد فیزیکی-اجتماعی) و شاخص ناپایداری لایسهلم (Lysholm) در فواصل پیش از تزریق، و ۳، ۶ و ۱۲ ماه پس از درمان انجام گرفت. نتایج نشان داد که معیارهای VAS و WOMAC پس از ۱۲ ماه بهبود معنیداری داشتند (به ترتیب $p<0.01$ و $p<0.05$). شاخص لایسهلم نیز در ماه دوازدهم بهبود فزایندهای نشان داد ($p>0.05$). هیچگونه عارضه جانبی جانبی در بیماران گزارش نشد. بر اساس یافتههای این مطالعه، یکبار تزریق PRS میتواند به عنوان یک استراتژی نوین بازسازی فاقد آنزیم، درد و سفتی مفصل را کاهش داده و عملکرد حرکتی را تا ۱۲ ماه بهبود ببخشد.
Platelet Rich STROMA, the Combination of PRP and tSVF and Its Potential Effect on Osteoarthritis of the Knee
Abstract
Background: Osteoarthritis (OA) of the knee is a degenerative disease accompanied by pain, reduced mobility, and a subsequent decrease in quality of life. Many studies on OA of the knee have reported that using an intercellular acting-derivate like platelet-rich plasma (PRP) results in a limited effect or none at all. The authors hypothesized that adding tissue-Stromal Vascular Fraction (tSVF) to PRP (Platelet Rich Stroma (PRS)) would reduce pain and improve functionality in osteoarthritis of the knee. Methods: A consecutive case series of fifteen patients (aged 43–75 years) suffering from OA of the knee (Kellgren–Lawrence stage two to three) were treated with a single injection of autologous PRS. tSVF was mechanically isolated by means of the fractionation of adipose tissue (FAT) procedure. Clinical evaluation was done using a visual analogue score (VAS), an adapted Western Ontario and McMaster Universities Osteoarthritis index (WOMAC), and a Lysholm score at fixed time points: pre-injection as well as three, six, and twelve months post-injection. Cartilage integrity and secondary abnormalities were tracked using T2 MRI evaluated by the Boston Leeds Osteoarthritis Knee Score (BLOKS). Results: VAS and WOMAC scores improved significantly after twelve months ( and ). Lysholm instability scores were also improved at twelve months () in comparison to pre-injection measurements. No complications were seen in any of the patients. One patient was excluded due to a total knee arthroplasty at 8 months. MRI analyses showed reduced presentation rates of synovitis and grade 3 cartilage defects, though not statistically significant. Conclusions: A single injection with PRS for OA of the knee seems to lead to an improvement of function and simultaneous reduction of pain and joint stiffness for a period of twelve months. Further controlled trials are required to determine the optimal treatment regimen and evaluate long-term results.
Keywords: SVF; PRP; knee osteoarthritis; regenerative medicine; stromal vascular fraction; adipose stem cells.
One-Page Core Scientific Breakdown
To facilitate swift data exploration, the architectural overview of this scientific trial is summarized in the unified profile below:
1. Introduction
Osteoarthritis (OA) of the knee stands as a chronic inflammatory, debilitating disease characterized by progressive degeneration of articular cartilage, persistent joint pain, structural deformities, and severe stiffness [1]. The clinical summation of these manifestations precipitates significantly compromised physical mobility and diminished socio-emotional quality of life [1,2]. Given the dual pressures of an aging global population and rising obesity rates across Western societies, the lifetime susceptibility metric for developing symptomatic knee OA sits at roughly 45% by age 85 [3]. Financially, the burden is massive; within American hospital networks in 2011, OA was documented as the second most expensive treated pathology, incurring health costs nearing $15 billion annually, with total knee arthroplasty (TKA) driving 50% of these admissions [4,5]. Projections indicate a 673% surge in TKA procedures within the United States by 2030, highlighting an urgent need for preventive, cost-efficient, and therapeutic strategies [6,7].
Current standard interventions remain predominantly restricted to pharmacological management (e.g., analgesics, non-steroidal anti-inflammatory drugs) or late-stage invasive surgeries [8,9]. Although TKA addresses end-stage joint degradation to restore movement, it carries postoperative risks—such as persistent pain, ambulatory deficits, and kneeling difficulties—alongside considerable economic expenditure and structural recovery downtimes averaging 12 weeks before returning to work [10,11]. Consequently, contemporary scientific interest has shifted toward autologous, low-cost regenerative therapies displaying minimal down-times, explicitly focusing on platelet-rich plasma (PRP) and stromal vascular fractions (SVF) [8,9,12].
PRP is isolated from whole autologous blood via centrifugation, optimally yielding a 2- to 2.5-fold expansion in baseline platelet counts [9]. Activated platelets unleash a cascade of vital growth factors, including transforming growth factor- (TGF-), insulin-like growth factor (IGF), and vascular endothelial growth factor (VEGF) [9]. These signaling elements stimulate the migration, mitotic expansion, differentiation, and angiogenic activation of resident mesenchymal stem cells or adipose-derived stromal cells (ASCs) [13,14].
ASCs represent multipotent stromal entities residing as precursor cells (such as pericytes and supra-adventitial elements) within the stromal vascular network of fat tissues [15,16]. Beyond ASCs, the native SVF heterogeneous matrix contains fibroblasts, endothelial components, periadventitial markers, and lymphocytes [12]. Isolation protocols follow either enzymatic or mechanical lines [17]. Enzymatic digestions yield cellular SVF (cSVF), a single-cell fluid suspension lacking native cell-to-cell structures or extracellular matrix (ECM) ties [17,18]. Conversely, non-enzymatic mechanical fractionation preserves tissue-like SVF (tSVF), excluding mature adipocytes while keeping the architectural ECM framework intact [17,18].
Mechanical tSVF isolation presents notable logistical advantages: it is less time-intensive, reduces operational costs, and avoids regulatory restrictions linked to chemical enzymes [17]. Biologically, the structural conservation of the ECM acts as a scaffold that facilitates a sustained, slow release of growth factors while supporting cell survival [19]. Together, these cellular arrays and growth factor complexes stimulate localized angiogenesis, drive parenchymal cell replication, decrease cellular apoptosis, and balance inflammatory pathways [17]. Because tissue inflammation and structural degradation form the foundation of OA pathology, tSVF shows strong potential for therapeutic tissue regeneration.
It was hypothesized that combining autologous PRP with mechanically isolated tSVF—forming an interactive autologous blend termed Platelet Rich Stroma (PRS)—would optimize joint signaling and offer an effective, synergistic treatment for knee OA. This paper presents a clinical case series evaluating 15 patients treated with a single local injection of PRS.
2. Material & Methods
2.1. Patient Population
Fifteen consecutive patients presenting with symptomatic knee OA were enrolled and treated between May 15, 2018, and October 9, 2018, by the chief investigator (HPS), in accordance with the ethical tenets of the Declaration of Helsinki. Patient referral, baseline grading, and longitudinal postoperative monitoring were managed independently by an orthopedic surgeon (RvD). Pathological inclusion required a definitive Grade 2 or Grade 3 assessment under the Kellgren–Lawrence radiographic classification scale.
Prior to enrollment, all candidates had experienced therapeutic failure with traditional conservative treatments, including prolonged physical therapy, intra-articular corticosteroid injections, and hyaluronic acid gel courses. Patients presenting with active malignancies, systemic sepsis, hematological or unstable hormonal disorders, active smoking histories, or undergoing antiaggregating systemic therapies were excluded. Every participant provided explicit, written informed consent prior to the procedure.
2.2. Preparation of Platelet-Rich Plasma
Autologous Conditioned Plasma (ACP)-PRP was prepared via a closed double-syringe architecture (Arthrex® ACP System, Naples, FL, USA). A 15 mL sample of peripheral venous blood was drawn from each patient without anti-coagulant additives. The collection system was placed within a swing-out rotor benchtop centrifuge (Hettich, Rotofix 32, Kirchenlengern, Germany) and spun at 1500 rpm (equivalent to 340 g) for 5 minutes at room temperature. Following phase separation, the isolated 5 cc plasma layer was drawn into the internal barrel of the double-syringe setup. This specific isolation framework provides a consistent 2- to 3-fold concentration expansion over baseline peripheral platelet levels [20].
2.3. Lipoharvesting and the Fractionation of Adipose Tissue (FAT) Procedure

Local anesthesia was achieved at the peri-umbilical donor zone via infiltration with a modified Klein solution containing 2% lidocaine, 1:200,000 epinephrine, and 6.8% sodium bicarbonate. A 30 cc volume of autologous lipoaspirate was harvested using dual Arthrex ACP syringes coupled with disposable surgical instruments from the Arthrex ACA kit.
The harvested lipoaspirate underwent an initial centrifugation phase at 2500 rpm (769 g) for 4 minutes. Following centrifugation, the upper lipid layer and lower aqueous fluid fractions were discarded. The remaining condensed adipose matter was consolidated into a single 10 cc luer-lock syringe using a 3-way stopcock system. This syringe was connected to a matched, empty 10 cc luer-lock syringe through a specialized single-hole disposable fractionator (aperture dimensions: 1 × 1.4 mm; Tulip Medical Systems, San Diego, CA, USA).
The mechanical Fractionation of Adipose Tissue (FAT) protocol was then performed by passing the adipose tissue back and forth through the fractionator port a total of 30 times [19,21]. This homogenized, mechanically disrupted fat tissue was returned to an ACP syringe and subjected to a second centrifugation round at 2500 rpm (769 g) for 2 minutes. This step separated an upper 90% oily fraction, which was decanted, leaving a concentrated 10% volumetric fraction (exactly 1 mL) of intact tissue-Stromal Vascular Fraction (tSVF) within the outer chamber of the ACP double-syringe assembly.
2.4. Platelet Rich Stroma (PRS) Injection
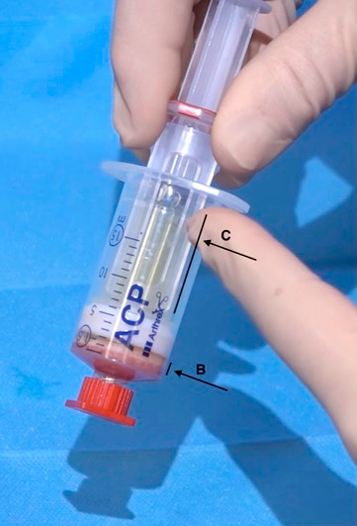
Following completion of the FAT mechanical protocol, the inner syringe of the tSVF assembly was replaced with the syringe containing the pre-isolated 5 cc of autologous PRP. The two autologous components were gently emulsified within a completely closed system without chemical reagents or digestive enzymes, yielding a final 6 cc volume of Platelet Rich Stroma (PRS). The entire extraction-to-formulation sequence was completed within 45 minutes.

The autologous PRS was administered under local anesthesia. The delivery protocol used a split-volume approach: 4 cc of the PRS mixture was delivered intra-articularly into the knee joint via a laterocranial retropatellar path, a technique validated for high intra-capsular targeting accuracy [22]. The remaining 2 cc of PRS was divided into equal 1 cc portions and injected peri-articularly into the soft tissues on both the medial and lateral margins of the patellar tendon at the level of the tibial plateau.
2.5. Evaluation of the Effect of PRS on Knee Osteoarthritis
Longitudinal clinical tracking was performed at pre-injection baseline, and at 3, 6, and 12 months post-injection. Objective and subjective changes were quantified via three validated clinical metrics:
-
Visual Analogue Scale (VAS): Administered to evaluate subjective pain levels at baseline, 2 weeks, 6 weeks, 3 months, 6 months, and 12 months post-procedure. Lower scores represent reduced pain.
-
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): Structured to evaluate three distinct symptom sub-scales: pain (5 items), joint stiffness (2 items), and socio-physical functionality (17 items). Individual domain metrics were converted into a standardized sum-score scale where higher final values indicate clinical improvement and superior outcomes.
-
Lysholm Instability Score: A validated 100-point questionnaire assessing knee-specific functional stability, mechanical locking, swelling, pain severity, stair climbing, and squatting capacity.
Structural evaluations of the joint were performed via T2-weighted Magnetic Resonance Imaging (MRI) scans at baseline and at the 6-month postoperative mark. Structural changes were scored independently using the Boston Leeds Osteoarthritis Knee Score (BLOKS) criteria, monitoring cartilage structural integrity, bone marrow lesions, osteophyte development, joint effusion, active synovitis, and meniscal degradation [23].
2.6. Statistical Analysis
Data groups were tested for a Gaussian normal distribution using the D’Agostino-Pearson omnibus test (). Longitudinal comparisons across matched, multi-temporal observation points were performed via repeated measures (RM) ANOVA ().
Post-hoc pairwise evaluations were conducted using Tukey’s multiple comparisons test (). All computational analyses and graphical processing were executed via GraphPad Prism software (Version 8.1.1 for OS X, GraphPad Software, San Diego, CA, USA). Continuous outcomes are presented as mean values standard deviations (SD).
3. Results
3.1. Patient Demographics
The consecutive clinical cohort comprised 15 patients (5 females, 10 males) with an age range of 43 to 75 years. Background history confirmed high rates of prior interventions: 12 patients had undergone intra-articular corticosteroid therapies, 10 had received hyaluronic acid viscosupplementation, and all reported chronic dependency on non-steroidal anti-inflammatory drugs (NSAIDs) alongside regular physical therapy protocols.
To isolate the therapeutic effects of the PRS injection, all concomitant interventions—including corticosteroids, specialized NSAID modifications, and physical therapy regimens—were suspended upon trial initiation. Out of the 15 primary participants, one male patient was excluded from the final 12-month analysis due to undergoing an elective total knee arthroplasty (TKA) at the 8-month postoperative mark.
3.2. Pain Significantly Decreased after Injection of PRS
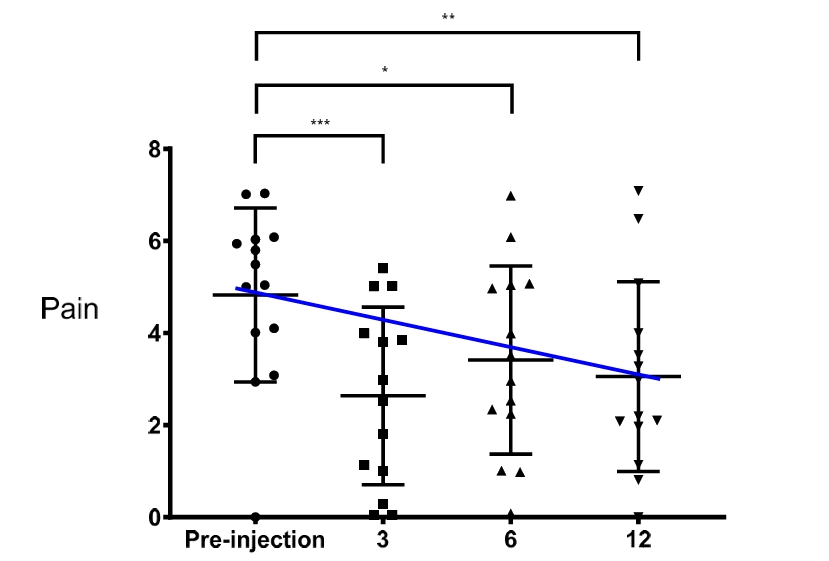
The longitudinal VAS pain dataset conformed to a normal distribution across all postoperative intervals, with the exception of the pre-injection baseline profile (). RM ANOVA confirmed that the observed reductions in pain variance were statistically significant and unlikely to result from random sampling error ().
The mean baseline VAS pain score decreased from an initial value of to at the 12-month final endpoint (). Between months 3 and 6, a minor, non-statistically significant upward trend in mean VAS pain score was observed before it decreased again toward the 12-month follow-up.
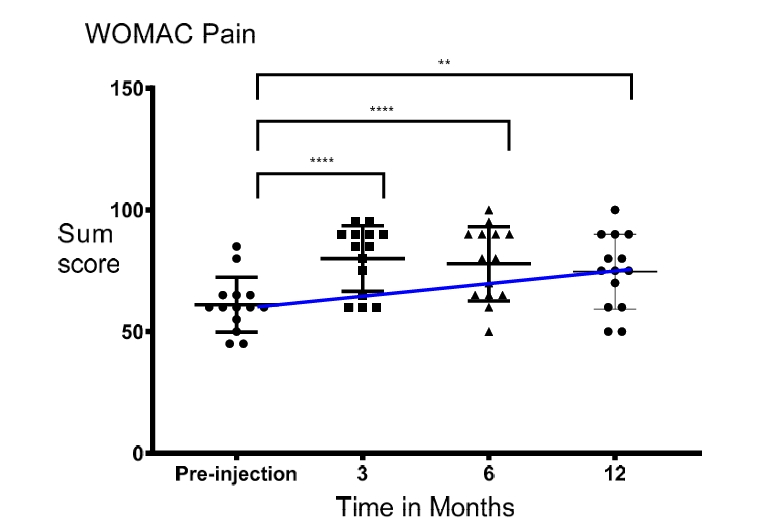
Analysis of the WOMAC pain sub-scale sum scores demonstrated normal distribution parameters () and significant overall variance over time (RM ANOVA, ). Mean baseline WOMAC pain scores improved from to a significantly improved status of at the 12-month mark ().
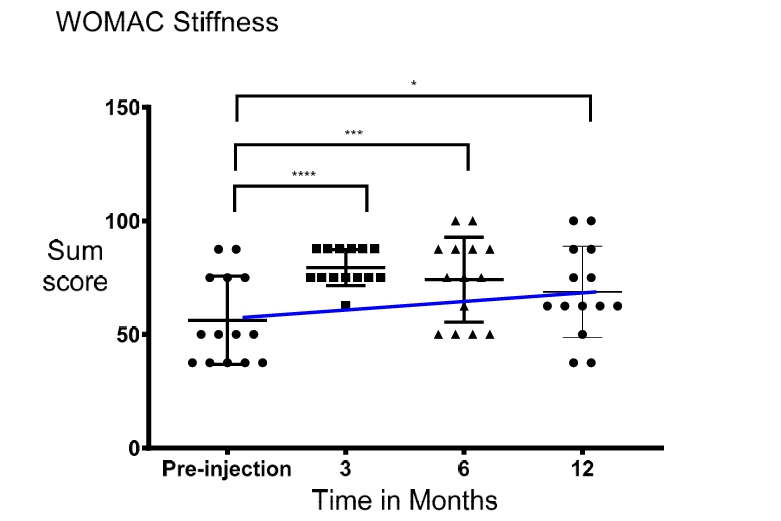
3.3. Functionality and Stiffness of the Knee Significantly Improved after Injection of PRS
WOMAC assessments for physical functionality and joint stiffness met all standard Gaussian distribution criteria (). RM ANOVA confirmed significant overall variation across timepoints for both functional metrics ().
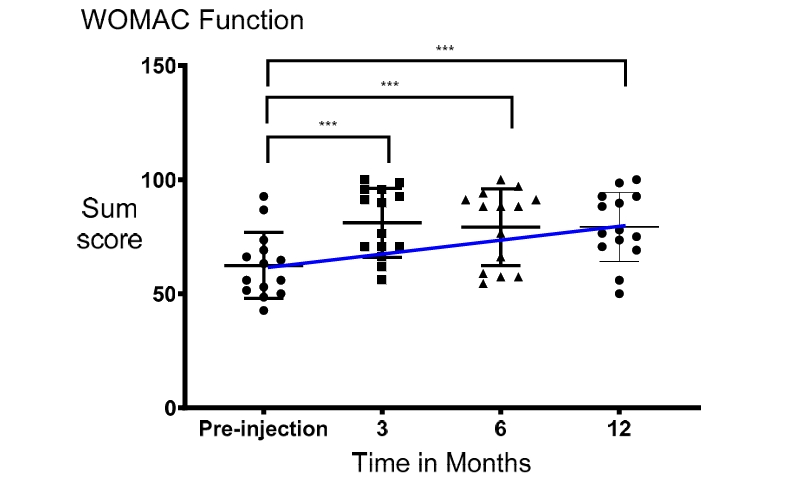
The mean WOMAC functionality sum score rose from a baseline value of to at the 12-month postoperative mark (). Parallel improvements were observed in joint stiffness parameters: the mean baseline WOMAC stiffness score improved from to by month 12 ().
The Lysholm structural instability metric followed a normal distribution () with a significant overall timeline shift (RM ANOVA, ). The cohort’s mean Lysholm functional score improved from an initial value of to at the 12-month follow-up ().
No clinical treatment down-time or severe adverse events were recorded within or around the treated knee joint across the patient cohort. Mild, self-limiting donor-site bruising and minor soreness resulting from the lipoharvesting procedure were reported by all patients, resolving spontaneously within 2 to 5 postoperative days.
A non-significant stabilization or slight decline in score trajectories was noted across the VAS and WOMAC pain and function scales between months 3 and 6. Similarly, non-significant downward trends occurred in WOMAC stiffness and Lysholm instability markers between months 3 to 12 and 6 to 12, respectively.
3.4. No Significant Changes on MRI Were Seen after Injection of PRS
Longitudinal structural evaluations using 2.0 Tesla MRI showed no statistically significant alterations in cartilage defects, subchondral bone marrow lesions, osteophyte growth, joint effusion, or meniscal tracking abnormalities.
However, positive structural trends were observed within specific sub-categories: the prevalence of Grade 3 cartilage defects within the medial tibiofemoral compartment decreased from 53% at baseline (8 out of 15 cases) to 42% at the 1-year mark (6 out of 14 cases). Additionally, the presence of active joint synovitis decreased from 60% at baseline (9 out of 15 cases) to 43% at 1 year post-injection (6 out of 14 cases).
4. Discussion
The findings of this consecutive case series indicate that a single autologous injection of PRS effectively reduces pain and joint stiffness while improving physical and socio-emotional functioning in patients with knee OA up to 12 months post-injection. The clinical data showed a rapid reduction in symptoms shortly after treatment. However, a minor recurrence of subjective discomfort was noted at the 6-month mark. This trend may stem from a spontaneous increase in physical activity around week 6, as initial pain relief allowed patients to resume physical tasks they had previously avoided. This pattern suggests that further research is needed to evaluate the timing and efficacy of serial injection protocols.
In healthy joints, articular chondrocytes maintain homeostatic balance within the extracellular matrix (ECM) by regulating the synthesis and degradation of structural proteins via growth factor and cytokine secretion [24]. In OA, this balance shifts toward matrix degradation driven by the overproduction of catabolic pro-inflammatory cytokines and proteolytic enzymes [25]. This metabolic imbalance induces cellular and oxidative stress, leading to cartilage degradation and chondrocyte apoptosis [26].
Stressed articular cells upregulate pro-inflammatory cytokines, including interleukin-1$\beta$ (IL-1$\beta$) and tumor necrosis factor-alpha (TNF-alpha), alongside endogenous damage-associated molecular patterns (DAMPs) [27]. The binding of these molecules to pattern-recognition receptors on chondrocytes activates the nuclear factor (NF$\kappa\beta$) signaling pathway [28], which drives inflammation, pain, and joint tissue degradation by promoting the secretion of matrix metalloproteinases (MMP-1, 3, 13) and ADAMTS4 [26].
Growth factors concentrated within PRP, such as hepatocyte growth factor, platelet-derived growth factor, IGF, and TGF-, can inhibit the NF$\kappa\beta$ cascade, thereby mitigating these anti-anabolic effects [26]. Downregulation of NF$\kappa\beta$ signaling has been shown to reduce ADAMTS4 production and promote the synthesis of type II collagen and proteoglycans in vitro [29,30]. This anti-inflammatory shift may reduce joint pain and help restore extracellular matrix homeostasis.
While various preclinical and clinical studies evaluating isolated PRP or SVF therapies have reported variable outcomes, interest in combining these modalities has recently grown [31–33]. The anti-inflammatory effects of PRP growth factors may be enhanced by adding non-enzymatically manipulated ASCs contained within tSVF. In tSVF, ASCs remain embedded in their native vascular fibrous matrix [19]. These stem cells also produce regenerative growth factors, including TGF- and IGF.
The combined delivery of PRP and matrix-bound ASCs may be essential for achieving a synergistic therapeutic effect. Platelet-secreted growth factors can bind directly to the tSVF matrix, allowing for sustained release during the healing phase [34]. Research by Willemsen et al. demonstrated that PRP induces a dose-dependent increase in ASC proliferation and upregulates paracrine genes such as TGF-, IGF, and fibroblast growth factor 1 (FGF1), while downregulating the pro-inflammatory gene IL-1$\beta$ [35].
This increase in anti-inflammatory signaling and reduction in catabolic cytokines may alleviate joint inflammation, while anti-apoptotic growth factors (IGF, FGF1) can reduce inflammatory cytokine secretion by chondrocytes. These insights suggest that maintaining non-manipulated ASCs within their native extracellular matrix (ECM) niche plays an important role in joint tissue regulation [34].
In this study, longitudinal MRI analysis did not demonstrate statistically significant improvements in synovitis or cartilage volume. This may be due to the small sample size or limitations in the 2.0 Tesla imaging system, which lacks the resolution needed to detect cell-level changes. Utilizing advanced cartilage-specific imaging software, which is often cost-prohibitive for standard clinical settings, might provide higher sensitivity.
Furthermore, clear evidence of in vivo cartilage regeneration in humans following SVF or PRP therapy remains limited. The observed clinical improvements may primarily result from an anti-inflammatory effect that lowers prostaglandin E2 levels within the joint, reducing pain sensation and improving function without requiring structural cartilage regeneration. Clinical symptoms, such as joint pain, frequently occur in patients without visible cartilage damage on imaging. These observations support the therapeutic strategy of preserving the “Trinity of Repair”—comprising signaling growth factors, repair cells (ASCs), and the structural ECM scaffold.
Due to the design limitations of this case series, a definitive synergistic effect between tSVF and PRP cannot be conclusively established, as the individual therapeutic contributions of tSVF or PRP could not be isolated [36]. Notably, the Lysholm instability score was the only functional metric that did not achieve statistical significance at 12 months. Prior research indicates that subjective joint instability does not correlate significantly with muscle strength or functional capacity [37].
Furthermore, reduced joint stiffness has been associated with an increased subjective perception of joint laxity [37]. Because WOMAC stiffness scores improved significantly by month 12, it is possible that reduced stiffness led patients to perceive greater joint instability during movement. This study highlights the need for larger, prospective, randomized controlled trials to evaluate PRS therapy against a control group (e.g., saline) to better characterize its clinical effects and differentiate them from placebo responses [38].
The clinical outcomes observed in this case series support the further evaluation of PRS for the management of knee OA, aligned with the clinical paradigm of “repair before replace.” Evaluating regenerative therapies for early- to mid-stage OA may offer a cost-effective strategy to improve quality of life and delay the need for joint replacement surgery.
References
لیست منابع شما را به همراه هایپرلینک مستقیم متصل به آدرس اصلی (با استفاده از فرمت استاندارد رفرنسدهی و لینکهای فعال پنهان در متن) آماده کردهام:
-
Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.L.; Protheroe, J.; Jordan, K.P. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507-515.
-
Day-Williams, A.G.; Southam, L.; Panoutsopoulou, K.; Rayner, N.W.; Esko, T.; Estrada, K.; Helgadottir, H.T.; Hofman, A.; Ingvarsson, T.; Jonsson, H.; et al. A variant in MCF2L is associated with osteoarthritis. Am. J. Hum. Genet. 2011, 89, 446-450.
-
Murphy, L.; Schwartz, T.A.; Helmick, C.G.; Renner, J.B.; Tudor, G.; Koch, G.; Dragomir, A.; Kalsbeek, W.; Luta, G.; Jordan, J.M. Lifetime risk of symptomatic knee osteoarthritis analysis and interpretation of data HHS public access. Arthritis Rheumatol. 2008, 59, 1207-1213.
-
Torio, C.M.; Andrews, R.M. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011: Statistical Brief #160. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006.
-
Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145-1153.
-
Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. Vol. 2007, 89, 780-785.
-
Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J. Impact of the economic downturn on total joint replacement demand in the United States: Updated projections to 2021. J. Bone Joint Surg. Am. Vol. 2014, 96, 624-630.
-
Filardo, G.; Kon, E.; Longo, U.G.; Madry, H.; Marchettini, P.; Marmotti, A.; Assche, D.V.; Zanon, G.; Peretti, G.M. Non-surgical treatments for the management of early osteoarthritis. Knee Surg. Sport Traumatol. Arthrosc. 2016, 24, 1775-1785.
-
Fibel, K.H. State-of-the-Art management of knee osteoarthritis. World J. Clin. Cases 2015, 3, 89.
-
Bala, A.; Penrose, C.T.; Seyler, T.M.; Mather, R.C.; Wellman, S.S.; Bolognesi, M.P. Outcomes after total knee arthroplasty for post-traumatic arthritis. Knee 2015, 22, 630-639.
-
Foote, J.A.J.; Smith, H.K.; Jonas, S.C.; Greenwood, R.; Weale, A.E. Return to work following knee arthroplasty. Knee 2010, 17, 19-22.
-
Gibbs, N.; Diamond, R.; Sekyere, E.O.; Thomas, W.D. Management of knee osteoarthritis by combined stromal vascular fraction cell therapy, platelet-rich plasma, and musculoskeletal exercises: A case series. J. Pain Res. 2015, 8, 799-806.
-
Tobita, M.; Tajima, S.; Mizuno, H. Adipose tissue-derived mesenchymal stem cells and platelet-rich plasma: Stem cell transplantation methods that enhance stemness Mesenchymal Stem/Stromal Cells-An update. Stem Cell Res. Ther. 2015, 6, 1-7.
-
Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641-648.
-
Corselli, M.; Chen, C.W.; Sun, B.; Yap, S.; Rubin, J.P.; Péault, B. The tunica adventitia of human arteries and veins as a source of mesenchymal stem cells. Stem Cells Dev. 2012, 21, 1299-1308.
-
Lin, G.; Garcia, M.; Ning, H.; Banie, L.; Guo, Y.-L.; Lue, T.F.; Lin, C.-S. Defining stem and progenitor cells within adipose tissue. Stem Cells Dev. 2008, 17, 1053-1063.
-
van Dongen, J.A.; Tuin, A.J.; Spiekman, M.; Jansma, J.; van der Lei, B.; Harmsen, M.C. Comparison of intraoperative procedures for isolation of clinical grade stromal vascular fraction for regenerative purposes: A systematic review. J. Tissue Eng. Regen Med. 2018, 12, e261-e274.
-
van Dongen, J.A.; Stevens, H.P.; Harmsen, M.C.; van der Lei, B. Mechanical micronization of lipoaspirates: Squeeze and emulsification techniques. Plast. Reconstr. Surg. 2017, 139, 1369e-1370e.
-
van Dongen, J.A.; Stevens, H.P.; Parvizi, M.; van der Lei, B.; Harmsen, M.C. The fractionation of adipose tissue procedure to obtain stromal vascular fractions for regenerative purposes. Wound Repair Regen. 2016, 24, 994-1003.
-
Mazzocca, A.D.; McCarthy, M.B.; Chowaniec, D.M.; Dugdale, E.M.; Hansen, D.; Cote, M.P.; Bardley, J.P.; Romeo, A.A.; Arciero, R.A.; Beitzelet, K. The positive effects of different platelet-rich plasma methods on human muscle, bone, and tendon cells. Am. J. Sports Med. 2012, 40, 1742-1749.
-
Van Dongen, J.A.; Gostelie, O.F.E.; Vonk, L.A.; De Bruijn, J.J.; Van Der Lei, B.; Harmsen, A.C.; Stevens, H.P. Fractionation of adipose tissue procedure with a disposable one-hole fractionator. Aesthet. Surg. J. 2019.
-
Maricar, N.; Parkes, M.J.; Callaghan, M.J.; Felson, D.T.; O’Neill, T.W. Where and how to inject the knee-A systematic review. Semin. Arthritis Rheum. 2013, 43, 195-203.
-
Hunter, D.J.; Lo, G.H.; Gale, D.; Grainger, A.J.; Guermazi, A.; Conaghan, P.G. The reliability of a new scoring system for knee osteoarthritis MRI and the validity of bone marrow lesion assessment: BLOKS (Boston-Leeds Osteoarthritis Knee Score). Ann. Rheum. Dis. 2008.
-
Sophia Fox, A.J.; Bedi, A.; Rodeo, S.A. The basic science of articular cartilage: Structure, composition, and function. Sports Health 2009, 1, 461-468.
-
Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786-801.
-
Andia, I.; Maffulli, N. Platelet-rich plasma for managing pain and inflammation in osteoarthritis. Nat. Rev. Rheumatol. 2013, 9, 721-730.
-
Chen, G.Y.; Nuñez, G. Sterile inflammation: Sensing and reacting to damage. Nat. Rev. Immunol. 2010, 10, 826-837.
-
Marcu, K.B.; Otero, M.; Olivotto, E.; Maria Borzi, R.; Goldring, M.B. NF-kappaB Signaling: Multiple angles to target OA. Curr. Drug Targets 2010, 11, 599-613.
-
Van Buul, G.M.; Koevoet, W.L.M.; Kops, N.; Bos, P.K.; Verhaar, J.A.; Weinans, H.; Bernsen, M.R.; van Osch, G.J. Platelet-rich plasma releasate inhibits inflammatory processes in osteoarthritic chondrocytes. Am. J. Sports Med. 2011, 39, 2362-2370.
-
Wu, C.C.; Chen, W.H.; Zao, B.; Lai, P.-L.; Lin, T.-C.; Lo, H.-Y.; Shieh, Y.-H.; Wu, C.-H.; Deng, W.-P. Regenerative potentials of platelet-rich plasma enhanced by collagen in retrieving pro-inflammatory cytokine-inhibited chondrogenesis. Biomaterials 2011, 32, 5847-5854.
-
Mehranfar, S.; Abdi Rad, I.; Mostafav, E.; Akbarzadeh, A. The use of stromal vascular fraction (SVF), platelet-rich plasma (PRP) and stem cells in the treatment of osteoarthritis: An overview of clinical trials. Artif. Cells Nanomed. Biotechnol. 2019, 47, 882-890.
-
Bansal, H.; Comella, K.; Leon, J.; Verma, P.; Agrawal, D.; Koka, P.; Ichim, T. Intra-Articular injection in the knee of adipose derived stromal cells (stromal vascular fraction) and platelet rich plasma for osteoarthritis. J. Transl. Med. 2017, 15, 141.
-
Hong, Z.; Chen, J.; Zhang, S.; Zhao, C.; Bi, M.; Chen, X.; Bi, Q. Intra-articular injection of autologous adipose-derived stromal vascular fractions for knee osteoarthritis: A double-blind randomized self-controlled trial. Int. Orthop. 2019, 43, 1123-1134.
-
van Dongen, J.A.; Getova, V.; Brouwer, L.A.; Liguori, G.R.; Sharma, P.K.; Stevens, H.P.; van der Lei, B.; Harmsen, M.C. Adipose tissue-derived extracellular matrix hydrogels as a release platform for secreted paracrine factors. J. Tissue Eng. Regen. Med. 2019, 13, 973-985.
-
Willemsen, J.C.N.; Spiekman, M.; Stevens, H.P.J.; Van Der Lei, B.; Harmsen, M.C. Platelet-Rich plasma influences expansion and paracrine function of adipose-derived stromal cells in a dose-dependent fashion. Plast. Reconstr. Surg. 2016, 137, 554e-565e.
-
Stevens, H.P.; Donners, S.; De Bruijn, J. Introducing platelet-rich stroma: Platelet-Rich Plasma (PRP) and Stromal Vascular Fraction (SVF) combined for the treatment of androgenetic alopecia. Aesthet. Surg. J. 2018, 38, 811-822.
-
Wallace, D.T.; Riches, P.E.; Picard, F. The assessment of instability in the osteoarthritic knee. EFORT Open Rev. 2019, 4, 70–76.
-
Saltzman, B.M.; Leroux, T.; Meyer, M.A.; Basques, B.A.; Chahal, J.; Bach, B.R., Jr.; Yanke, A.B.; Cole, B.J. The therapeutic effect of intra-articular normal saline injections for knee osteoarthritis: A meta-analysis of evidence level 1 studies. Am. J. Sports Med. 2017, 45, 2647-2653.