مقدمه: استئوآرتریت (OA) یکی از شایعترین اختلالات مزمن مفصلی است که با تخریب غضروف آرتیکولار و التهاب سینوویال همراه است. درمانهای سنتی مانند مسکنها دارویی و فیزیوتراپی معمولاً موقتی بوده و سیر پیشرفت بیماری را متوقف نمیکنند. پزشکی بازسازیکننده با تکیه بر ترکیب فراکشن عروقی استرومال (SVF) حاصل از بافت چربی و فیبرین غنی از پلاکت (PRF) مشتق از خون بیمار، رویکرد نوینی برای بازسازی بافت مفصل فراهم کرده است. هدف این مطالعه، ارزیابی نتایج بالینی و رادیوگرافیک دو ساله این درمان ترکیبی در بیماران مبتلا به آرتروز زانو و لگن است.
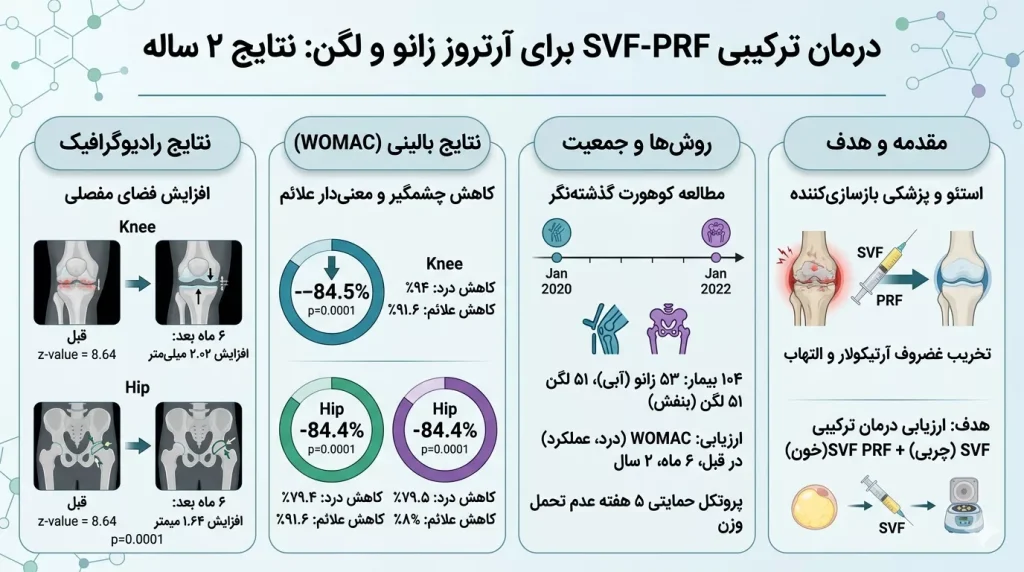
روشها: این پژوهش یک مطالعه کوهورت گذشتهنگر بر روی دادههای بالینی ۱۰۴ بیمار (۵۳ بیمار مبتلا به آرتروز زانو و ۵۱ بیمار مبتلا به آرتروز لگن) است که بین ژانویه ۲۰۲۰ تا ژانویه ۲۰۲۲ تحت درمان قرار گرفتهاند. ارزیابی میزان بهبود علائم بالینی (درد، خشکی مفصل و عملکرد فیزیکی) با شاخص WOMAC در بازههای زمانی قبل از درمان، ۶ ماه و ۲ سال بعد انجام شد. همچنین تغییرات رادیوگرافیک فضای مفصلی قبل از درمان و ۶ ماه پس از آن مورد تحلیل قرار گرفت. پس از تزریق، پروتکل حمایتی شامل ۵ هفته عدم تحمل وزن بر روی مفصل اجرا گردید.
نتایج: پس از ۲ سال، کاهش چشمگیر و معنیداری در نمرات شاخص WOMAC برای هر دو گروه زانو (۸۴.۵٪ کاهش نمره کل) و لگن (۸۴.۴٪ کاهش نمره کل) مشاهده شد (p=0.0001). میزان درد در زانو ۹۴٪ و در لگن ۷۹.۵٪ کاهش یافت. تحلیل تصاویر رادیوگرافیک نیز افزایش معنیداری در فضای مفصلی نشان داد؛ میانگین افزایش فضای مفصل در زانو ۲.۰۲ میلیمتر و در لگن ۱.۶۴ میلیمتر بود (p=0.0001).
نتیجهگیری: درمان ترکیبی SVF و PRF به عنوان یک روش کمتهاجمی و ایمن، کارایی بالایی در کاهش طولانیمدت علائم بالینی و افزایش بازسازی غضروف در بیماران مبتلا به استئوآرتریت زانو و لگن دارد و میتواند به عنوان جایگزینی مناسب برای جراحی تعویض مفصل مطرح شود.
Stromal Vascular Fraction with Platelet-Rich Fibrin for Osteoarthritis Management in Knee and Hip Osteoarthritis: A Retrospective 2-Year Follow-Up Study
Author: Torbjörn Ogéus DC, PgD, MSc
Affiliation: Stockholms led- & smärtklinik, 11424, Stockholm, Sweden
Abstract
Introduction: In recent years, regenerative medicine has emerged as a promising frontier in the management of various musculoskeletal disorders, including osteoarthritis (OA). Among the plethora of regenerative therapies, stromal vascular fraction (SVF) therapy combined with platelet-rich fibrin (PRF) has garnered significant attention for its potential to mitigate OA progression and promote joint regeneration.
Methods: This is a retrospective database cohort study. The clinic database was searched for patients that had undergone SVF and PRF for hip- or knee OA between January 2020 and January 2022. 104 patients were included in the study. The analyzed data were 2-year follow-up WOMAC scores and radiographic pictures before and 6 months after the treatment.
Results: Statistically significant positive changes on WOMAC scores (p = 0.0001) were presented for both hip- and knee OA. Radiographic increase of joint space in the treated joints were presented; a mean increase of 2 mm for knees and 1.6 mm for hip joints (p = 0.0001).
Conclusion: SVF combined with PRF is an effective treatment for hip- and knee osteoarthritis. Significantly lowered WOMAC scores 2 years after the treatment, combined with a significant radiographic increase in joint space were presented.
Keywords: Stem cell; SVF; PRF; Regenerative medicine; Knee; Hip; Osteoarthritis; Radiographic WOMAC
Abbreviations:
-
OA: Osteoarthritis
-
SVF: Stromal Vascular Fraction
-
PRF: Platelet Rich Fibrin
-
WOMAC: Western Ontario and McMaster Universities Arthritis Index
-
NSAIDs: Nonsteroidal Anti-inflammatory Drugs
-
MSC: Mesenchymal Stem Cells
-
TGF-β: Transforming Growth Factor-beta
-
PDGF: Platelet-derived Growth Factor
-
PPP: Platelet-poor Plasma
-
ALB-PRF: Heat Coagulated Albumin-PRF
-
C-PRF: Concentrated PRF
-
SD: Standard Deviation
-
ROM: Range of Motion
1. Introduction
Osteoarthritis (OA) stands as a prevalent chronic joint disorder characterized by progressive degeneration of articular cartilage, subchondral bone alterations, and synovial inflammation. With an aging population and increasing rates of obesity worldwide, the burden of OA continues to escalate, posing substantial challenges to healthcare systems globally. Traditional management strategies such as nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and ultimately joint replacement surgeries offer symptomatic relief but often fall short in halting disease progression or providing long-term benefits. Hence, there exists a pressing need for innovative therapeutic modalities that not only alleviate symptoms but also address the underlying pathophysiological mechanisms driving OA.
In recent years, regenerative medicine has emerged as a promising frontier in the management of various musculoskeletal disorders, including OA. Among the plethora of regenerative therapies, stromal vascular fraction (SVF) therapy combined with platelet-rich fibrin (PRF) has garnered significant attention for its potential to mitigate OA progression and promote joint regeneration. SVF, a heterogeneous cell population derived from adipose tissue, harbors mesenchymal stem cells (MSCs), endothelial progenitor cells, and various growth factors. PRF, on the other hand, is a concentrate of platelets and leukocytes obtained from the patient’s own blood, rich in bioactive molecules such as transforming growth factor-beta (TGF-β) and platelet-derived growth factor (PDGF). When administered in combination, SVF and PRF exhibit synergistic effects, harnessing the regenerative capacity of both cell-based and growth factor-mediated approaches.
In 2014, data on cartilage regrowth was presented after a single dose of Mesenchymal stem cells injected in knees, using arthroscopic before- and after pictures. To our knowledge, no previous long-term data has been published on a combination of SVF and PRF treatment in knee and hip osteoarthritis. This study presents 2-year follow-up data from 104 patients with hip and knee OA that sheds light on the regenerative potential of SVF combined with PRF as a novel therapeutic paradigm for OA management.
2. Materials and Methods
2.1. Protocol Context and Rationale
Various types of autologous platelet concentration protocols have been proposed to be used to treat osteoarthritis and cartilage defects. Some studies have indicated a positive effect on pain, function, and stiffness symptoms; however, the effect of injected platelets in the injured joint might require multiple injections and no standard protocols exist. One way of extending the effect of the injected platelets is to heat a liquid platelet-poor plasma (PPP) layer; the resorption properties of heated albumin (albumin gel) can thereby be extended from 2 weeks to greater than 4 months (ALB-PRF).
The use of autologous mesenchymal stem cells harvested from the Stromal Vascular Fraction (SVF) has been used increasingly in the treatment of osteoarthritis with promising results in cartilage repair. The combination of autologous blood products such as PRF intra-articularly has shown beneficial effects for OA treatment.
2.2. Preparation of PRF, ALB-PRF, and SVF
All patients that underwent SVF and PRF treatment of hip- and knee OA at the clinic during the reported time frame received the same treatment protocol:
-
Blood Collection & Centrifugation: 40ml of blood was collected from the patients before each of the PRF injections. Four 10ml plastic, round-bottomed vacuum tubes (Liquid PRF tubes) were used to collect the blood. After collection, the tubes were spun on a horizontal swing-out bucket rotors centrifuge system.
-
PRF Formulations: Two PRF protocols were utilized following international guidelines published by Miron et al. in 2019. The Concentrated-PRF (C-PRF) injection consisted of 4ml centrifuged at 2000×g for 8 min. The Albumin Gel-PRF (ALB-PRF) injections consisted of 5ml centrifuged at 2000×g for 8 min on a horizontal centrifuge; the isolated albumin layer was subsequently heated at 75°C for 10 min. Finally, the heat-coagulated albumin gel was cooled down to room temperature and mixed with the remaining C-PRF to create the final ALB-PRF matrix. The Bio-PRF horizontal centrifuge (Bio-PRF, USA) was used for all blood preparations.
-
SVF Isolation: The SVF preparation followed the MyStem™ system protocol (MyStem evo Bi-Medica, Treviolo, Italy). From the abdomen, 80 ml of adipose tissue was harvested via liposuction and introduced into the MyStem closed filtration system. Following standardized filtration and wash cycles, the residual fluids and oils were meticulously separated, yielding a 10 ml concentrated autologous SVF suspension prepared for immediate injection.
2.3. Administration Protocol and Post-Treatment Rehabilitation
The clinical timeline comprised a multi-step intra-articular series utilizing ultrasound guidance for accurate needle placement inside the joint capsule:
-
Week 1: An initial C-PRF injection was administered 2 days prior to the primary SVF deployment.
-
Week 2: Two separate C-PRF injections were given, spaced 2 days apart.
-
Final Step: The series concluded with a localized delivery of the extended-release ALB-PRF complex.
Following the SVF intervention, patients were instructed to strictly avoid weight-bearing on the treated joint for 5 weeks using supportive crutches. Once the non-weight-bearing phase successfully concluded, all subjects underwent a progressive home rehabilitation scheme consisting of stationary bicycling for 15 minutes daily alongside light resistance training with structured weekly increments.
2.4. Study Design and Selection Criteria
This study is structured as a retrospective database cohort study. According to the guidelines set by the Ethics Commission of Stockholm, Sweden, retrospective database studies treating anonymized sets do not require individual informed consent or formal ethical approval.
The clinic registry noted 123 patients (58 female and 65 male) who originally underwent the therapy series within the tracking interval. On treatment day 1, baseline registry details were logged with written patient consent.
-
Inclusion Criteria: Patients scheduled for joint-specific SVF/PRF treatment with complete Western Ontario and McMaster Universities Arthritis Index (WOMAC) documentation across all target milestones (Baseline, 6 Months, 2 Years).
-
Exclusion Criteria: Patients lacking any segment of the longitudinal follow-up surveys or those failing to maintain compliance during the post-procedural 5-week non-weight-bearing timeline.
A final total of 104 patients successfully fulfilled the tracking criteria (50 female, 54 male). The population was distributed into 53 patients evaluated for knee OA and 51 patients evaluated for hip OA.
2.5. Clinical and Radiographic Outcome Inventories
-
The WOMAC Survey Instrument: Patients completed the standardized self-administered survey (taking 5–10 minutes) across 24 distinct parameters mapping Pain (5 items), Stiffness (2 items), and Physical Function (17 items). Utilizing a 5-point Likert scale (0–4), lower score outputs represent diminished symptomatic severity and lesser clinical disability. Dimensional bounds restrict subscale sums to maximum capacities of 20 points (Pain), 8 points (Stiffness), and 68 points (Physical Function), summarizing into a global index score.
-
Digital Radiographic Database: Standardized radiographs of the targeted joints were secured at baseline and at the 6-month interval. The localized articular joint space width was quantified digitally in millimeters (mm) to calculate longitudinal cartilage/structural modifications.
2.6. Statistical Analysis
Sample metrics were characterized through mean calculations paired with standard deviations ( SD). Normal data distribution configurations were assessed utilizing T-tests and Analysis of Variance (ANOVA) routines. Pairwise multiple comparisons across intervals were completed via independent t-tests utilizing Prism 10 for Windows (Microsoft, USA). The alpha value defining statistical significance thresholds was set at .
3. Results
3.1. Demographic Profiles
The integrated study collective presented an average age profile of years. No statistically significant variations were identified between the separate knee and hip groups regarding age boundaries () or gender distributions ().
Table 1: Demographic data of the patients in the sample.
3.2. WOMAC Longitudinal Clinical Outcomes
Statistical analysis revealed significant clinical improvements across all tracked dimensions over the 24-month horizon:
-
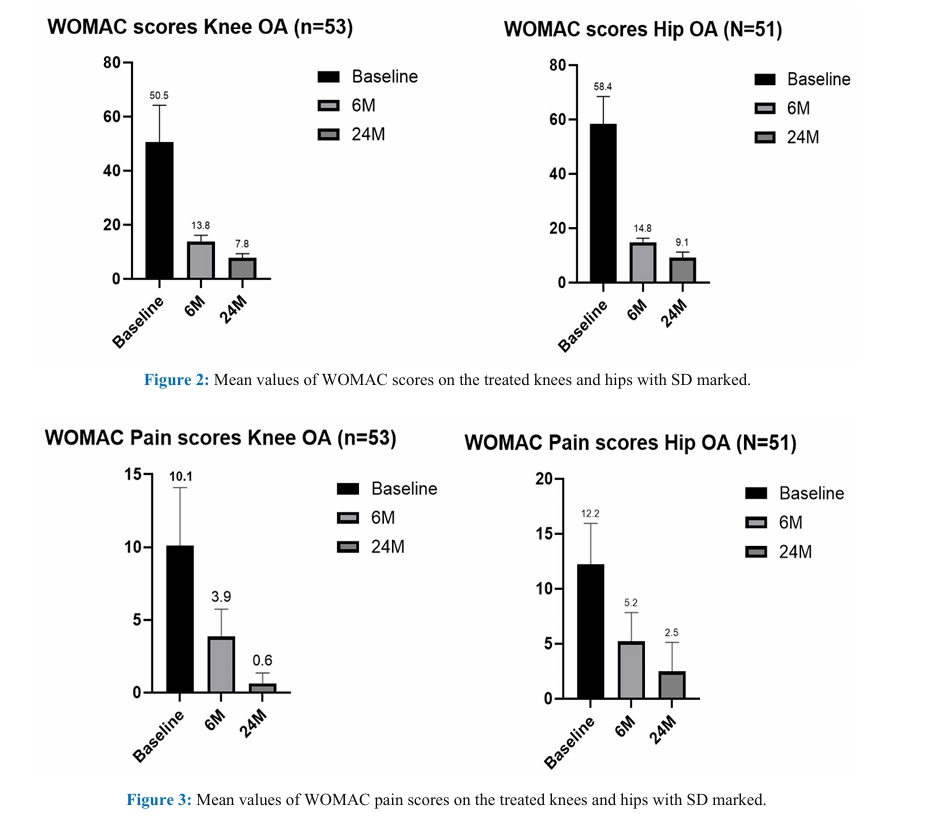
Global index WOMAC Scores: The knee cohort exhibited a significant reduction () from a mean baseline of 50.5 to 13.8 at 6 months, and finally down to 7.8 at 2 years, marking an overall 84.5% relief pattern. The hip collective displayed a parallel significant downward path (), shifting from a baseline mean of 58.4 to 14.8 at 6 months, and arriving at 9.1 at the 2-year tracking window (an 84.4% cumulative improvement).
-
Pain Dimensions: Knee localized pain levels demonstrated a 94% decrease (), dropping from 10.1 (baseline) to 3.9 (6 months), and down to 0.6 at 24 months. Hip localized pain metrics altered significantly () from 12.2 at baseline to 5.2 at 6 months, and down to 2.5 at 24 months (a 79.5% reduction).
-
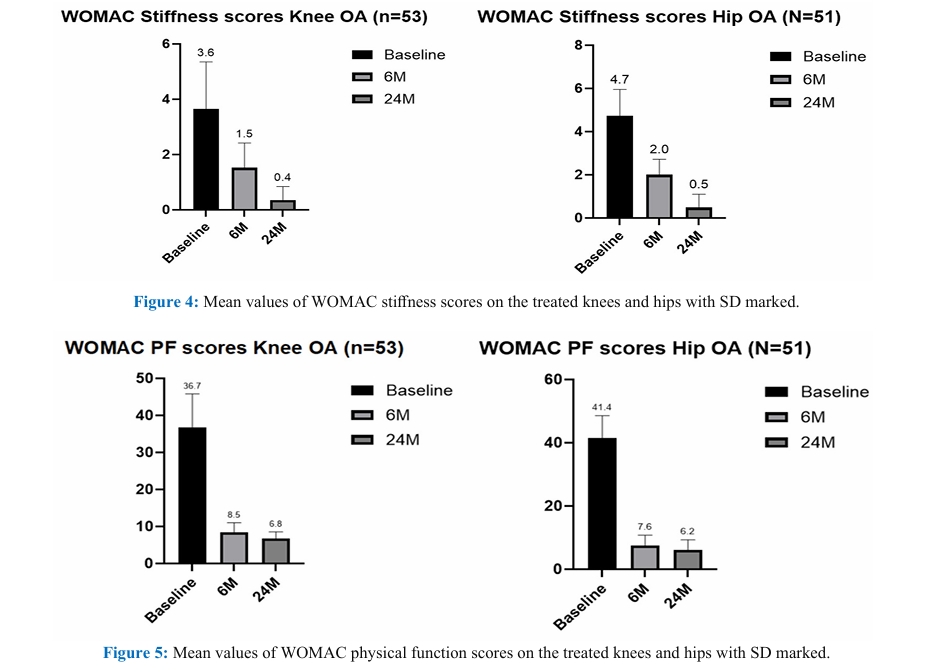
Stiffness Scales: Both articular cohorts registered matching 89% improvements () across 2 years. Knee tracking scores altered from 3.6 to 0.4, while hip stiffness indexes dropped from 4.7 to 0.5.
-
Physical Function Metrics: Knee function indices improved by 81% over 24 months (shifting from 36.7 down to 6.8, ). Concurrently, the hip cohort experienced a significant 85% functional advancement, shifting from 41.4 at baseline to 7.6 at 6 months, and resolving at 6.2 at 2 years ().
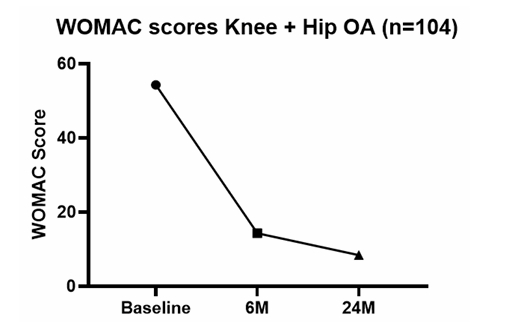
When compiling the metrics of all 104 treated patients across both joints, the total combined cohort displayed a statistically significant () overall WOMAC score improvement of 84.5%, dropping from a baseline mean of 54.3 to 8.4 at the 2-year mark. No statistically significant disparities were observed between genders across any metric dimension.
3.3. Objective Radiographic Data
Using a two-tailed unpaired T-test to analyze pre- and post-treatment images, both groups showed a statistically significant expansion in joint space width at the 6-month tracking milestone.
-
Knee OA Joints: Displayed a mean joint space width expansion of 2.02 mm ().
-
Hip OA Joints: Demonstrated a mean joint space width expansion of 1.64 mm ().
4. Discussion
The clinical data detailed here demonstrates a highly successful novel application of combined SVF, C-PRF, and ALB-PRF. This offers an effective alternative intervention for patients when conservative medication strategies fail or as an option prior to aggressive surgical joint replacement. While standalone SVF or platelet treatments have shown a growing body of evidence for short-term symptom relief in knee OA, long-term combinations have remained largely unaddressed.
In this study, both tracked joint cohorts demonstrated substantial clinical progress, though knee joints achieved slightly better overall improvements compared to hip joints across all WOMAC domains. This clinical variation aligns with the radiographic outcomes, which showed a slightly smaller joint space increase in hip joints (1.64 mm vs. 2.02 mm). This pattern is anatomically logical given that the baseline joint space and cartilage thickness of the hip are naturally smaller than those of the knee.
هماهنگی جالب توجهی میان نمرات بهبود یافته شاخص WOMAC در این روش با نتایج تاریخی جراحی تعویض کامل مفصل وجود دارد. با این حال، الگوهای بازیابی پس از تعویض مفصل معمولاً وارونه است؛ بیماران جراحی تعویض لگن سریعتر بهبود یافته و نمرات بهتری نسبت به زانو کسب میکنند. علاوه بر این، در حالی که نتایج جراحی به سرعت نمایان میشود، این رویکرد سلولی اتولوگ برای نشان دادن کامل پتانسیل درمانی خود به زمان بیشتری نیاز دارد و نتایج حداکثری آن به جای ۶ ماه، در بازه زمانی ۲ ساله تثبیت میگردد. این امر شواهد مهمی از پایداری طولانیمدت درمان ارائه میدهد و شکافهای موجود در ادبیات پیشین را که عمدتاً بر دادههای یکساله متمرکز بودند، برطرف میکند.
For patients who did not achieve their full clinical expectations despite showing measurable improvement, this therapy still offered a clear benefit by delaying the need for total joint arthroplasty. This delay is particularly valuable for younger individuals with severe OA, who are often advised to postpone joint replacement to avoid the long-term complications associated with implant wear and revision surgeries.
A key advantage of this protocol is its minimally invasive, autologous nature. Using the patient’s own tissue minimizes the risk of a rejection reaction. While some studies support the use of repeated injections, others show no added benefit from booster doses. Furthermore, recent evidence warns that frequent, repeated injections of adipose-derived stem cells may trigger anti-histone H2B antibody production, risking severe secondary arthritis and joint degeneration. This highlights the clinical value of our protocol, which achieves lasting 2-year therapeutic efficacy through a single, structured sequence.
Study Limitations
-
Lack of Kinematic Range Data: Perceived joint mobility was captured well via WOMAC domains, but the study lacked direct goniometric data measuring joint range of motion (ROM) in degrees, which would be particularly informative for hip OA.
-
Imaging Constraints: Standard radiographs provided clear objective measurements of joint space width at a reasonable cost, but future studies would benefit from pre- and post-treatment magnetic resonance imaging (MRI) to directly assess structural changes within cartilage lesions.
-
Potential Selection Bias: The strict exclusion of patients who failed to adhere to the post-injection 5-week non-weight-bearing phase means valuable data is missing. It remains unanswered whether the observed joint space expansion and clinical success depend entirely on this non-weight-bearing rehabilitation phase.
-
Methodological Design: The retrospective nature of this study and the absence of a parallel control or placebo group limit the ability to completely rule out confounding factors. Larger randomized controlled trials are required to firmly establish efficacy compared to alternative therapies.
5. Conclusion
In conclusion, SVF combined with PRF is an effective, low-risk, and minimally invasive treatment for both hip and knee osteoarthritis. The protocol delivers a statistically significant reduction in clinical symptoms that persists for at least 2 years post-treatment, accompanied by a significant objective increase in radiographic joint space width. These findings support this combined autologous therapy as a viable clinical alternative to total joint replacement surgery for managing progressive osteoarthritis.
6. Declarations
-
Ethics Approval: According to the Ethics Commission of Stockholm, Sweden, retrospective database-based studies do not require formal ethical approval and patient informed consent whenever data are acquired, saved, and treated anonymously. This study was conducted in full accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
-
Consent for Publication: Not applicable. All data exposed in this manuscript was completely anonymized and contains no individual identifying details.
-
Funding: The author received no financial support for the research, authorship, and/or publication of this article.
-
Competing Interests: The author declares that he has no competing interests.
-
Authors’ Contributions: All texts, design, literature review, and drafting of this study were performed by TO.
-
Availability of Data and Materials: All data generated or analyzed during this study can be provided by the corresponding author upon reasonable request.
7. References
-
Loeser RF, Goldring SR, Scanzello CR, et al. Osteoarthritis: A Disease of the Joint as an Organ. Arthritis & Rheumatism 64 (2012): 1697-1707.
-
Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis and Cartilage 27 (2019): 1578-1589.
-
Pak J. Regeneration of human bones in hip osteonecrosis and human cartilage in knee osteoarthritis with autologous adipose-tissue-derived stem cells: a case series. Journal of Medical Case Reports 5 (2011): 296.
-
Zuk PA, Zhu M, Ashjian P, et al. Human Adipose Tissue Is a Source of Multipotent Stem Cells. Molecular Biology of the Cell 13 (2002): 4279-4295.
-
Dohan DM, Choukroun J, Diss A, et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part I: technological concepts and evolution. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 101 (2006): e37-e44.
-
Jo CH, Lee YG, Shin WH, et al. Intra-articular injection of mesenchymal stem cells for the treatment of osteoarthritis of the knee: a proof-of-concept clinical trial. Stem Cells 32 (2014): 1254-1266.
-
Costa LAV, Lenza M, Irrgang JJ, et al. How Does Platelet-Rich Plasma Compare Clinically to Other Therapies in the Treatment of Knee Osteoarthritis? A Systematic Review and Meta-analysis. Am J Sports Med 51 (2023): 1074-1086.
-
Fujioka-Kobayashi M, Schaller B, Mourão CFAB, et al. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets 32 (2021): 74-81.
-
Mehranfar S, Abdi Rad I, Mostafavi E, et al. The use of stromal vascular fraction (SVF), platelet-rich plasma (PRP) and stem cells in the treatment of osteoarthritis: an overview of clinical trials. Artif Cells Nanomed Biotechnol 47 (2019): 882-890.
-
Miron RJ, Pinto NR, Quirynen M, et al. Standardization of relative centrifugal forces in studies related to platelet-rich fibrin. Journal of Periodontology 90 (2019): 817-820.
-
Fujioka-Kobayashi M, Katagiri H, Kono M, et al. Improved growth factor delivery and cellular activity using concentrated platelet-rich fibrin (C-PRF) when compared with traditional injectable (i-PRF) protocols. Clin Oral Investig 24 (2020): 4373-4383.
-
Miron RJ, Pikos MA, Estrin NE, et al. Extended platelet-rich fibrin. Periodontol 2000 (2023).
-
Ackerman I. Western Ontario and McMaster universities osteoarthritis index (WOMAC). Aust J Physiother 55 (2009): 213.
-
McConnell S, Kolopack P, Davis AM. The western Ontario and McMaster universities osteoarthritis index (WOMAC): a review of its utility and measurement properties. Arthritis Rheum 45 (2001): 453-461.
-
Di Matteo B, Vandenbulcke F, Vitale ND, et al. Minimally Manipulated Mesenchymal Stem Cells for the Treatment of Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Stem Cells Int 2019 (2019): 1735242.
-
Marques CJ, Pinnschmidt HO, Bohlen K, et al. TKA patients experience less improvement than THA patients at 3 and 12 months after surgery. A retrospective observational cohort study. J Orthop 21 (2020): 517-522.
-
Naal FD, Impellizzeri FM, Lenze U, et al. Clinical improvement and satisfaction after total joint replacement: a prospective 12-month evaluation on the patients’ perspective. Qual Life Res 24 (2015): 2917-2925.
-
Anil U, Markus DH, Hurley ET, et al. The efficacy of intra-articular injections in the treatment of knee osteoarthritis: A network meta-analysis of randomized controlled trials. Knee 32 (2021): 173-182.
-
Fraenkel L, Suter L, Weis L, et al. Variability in recommendations for total knee arthroplasty among rheumatologists and orthopedic surgeons. J Rheumatol 41 (2014): 47-52.
-
Yang Y, Lan Z, Yan J, et al. Effect of intra-knee injection of autologous adipose stem cells or mesenchymal vascular components on short-term outcomes in patients with knee osteoarthritis: an updated meta-analysis of randomized controlled trials. Arthritis Res Ther 25 (2023): 147.
-
Yokota N, Lyman S, Hanai H, et al. Clinical Safety and Effectiveness of Adipose-Derived Stromal Cell vs Stromal Vascular Fraction Injection for Treatment of Knee Osteoarthritis: 2-Year Results of Parallel Single-Arm Trials. Am J Sports Med 50 (2022): 2659-2668.
-
Hosono Y, Kuwasawa A, Toyoda E, et al. Multiple intra-articular injections with adipose-derived stem cells for knee osteoarthritis cause severe arthritis with anti-histone H2B antibody production. Regen Ther 24 (2023): 147-153.
-
Fujita M, Matsumoto T, Sobajima S, et al. Clinical and Radiological Comparison of Single and Double Intra-articular Injection of Adipose-Derived Stromal Vascular Fraction for Knee Osteoarthritis. Cell Transplant 32 (2023): 9636897231190175.
-
Zhang Y, Bi Q, Luo J, et al. The Effect of Autologous Adipose-Derived Stromal Vascular Fractions on Cartilage Regeneration Was Quantitatively Evaluated Based on the 3D-FS-SPGR Sequence: A Clinical Trial Study. Biomed Res Int 2022 (2022): 2777568.
-
Mazini L, Rochette L, Amine M, et al. Regenerative Capacity of Adipose Derived Stem Cells (ADSCs), Comparison with Mesenchymal Stem Cells (MSCs). Int J Mol Sci 20 (2019): 2523.
-
Rebelatto CK, Aguiar AM, Moretão MP, et al. Dissimilar differentiation of mesenchymal stem cells from bone marrow, umbilical cord blood, and adipose tissue. Exp Biol Med (Maywood) 233 (2008): 901-913.
-
Aletto C, Oliva F, Maffulli N. Knee intra-articular administration of stromal vascular fraction obtained from adipose tissue: A systematic review. J Clin Orthop Trauma 25 (2022): 101773.
-
Onoi Y, Matsumoto T, Sobajima S, et al. Clinical use of autologous adipose-derived stromal vascular fraction cell injections for hip osteoarthritis. Regen Ther 24 (2023): 94-102.
-
Tsubosaka M, Matsumoto T, Sobajima S, et al. Comparison of Clinical and Imaging Outcomes of Different Doses of autologous adipose-derived stromal vascular fraction cell injections for knee osteoarthritis. Regen Ther 24 (2023).